Abstract
Globally, health management information systems (HMIS) in strengthening health systems have gained recognition due to potential of technology to improve access to quality care in underserved communities. In Kenya, the functionality of Community based- Health Management Information System (CBHMIS) currently stands at 55% down from 64% in year 2015. The aim of this paper was to determine the influence of behavioral factors of community units personnel on CBHMIS. As a nested study, with a broader aimt to establish the operational status of CBHMIS and its use in selected counties in Kenya; The main objective of this research was: To establish whether behavioural factors of Community Health Promoters (CHPs) influence CBHMIS use in Kenya. A mixed method design. was adopted, Kiambu, Kajiado and Nairobi counties formed the study location, a target population of 156 active community units was considered to arrive at a total sample of 122 community units and out of 7800CHPs a sample of 366 respondents was drawn. Multistage sampling was used to identify the CUs, and systematic random sampling to identify 366 respondents. Quantitative data tools were semi-structured closed ended questionnaires. Qualitative data tools included observation checklist, Focus Group Discussion and Key Informant Interviews guides. Quantitative data was analyzed using SPSS to generate univariate and bivariate analysis at p<0.05 significance level; Qualitative data was analyzed using content analysis based on key themes generated from the objectives. Results were presented in form of graphs, tables, figures, and narration. This study showed that the use of Community based- Health Management Information System stood at 56.6%. Behavioural factors were found to significantly influence use of Community based- Health Management Information System. Further, of the total variations in the use of Community based- Health Management Information System, behavioral factor explains 13.7% (R2 = .137). Results show that the model was valid (F(1, 363) = 58.579, P = .001) hence the explanatory variable (X2, Behavioral factors) is good in explaining total variations in Use of CbHMIS by community units. This implies that the use of CbHMIS by Community Units (CU) improves significantly when the community units have better behavioural factors. In conclusion, behavioural factors of CHPs have strong and significant influence on the CBHMIS use. Motivation of CHPs is key as a motivator to CBHMIS use, as well as. provision of material support including reporting tools and IEC materials and capacity development technical, computer and electronic reporting skills to enhamce CHP operations and processes.
Keywords
Health System Strengthening, Health Management Information Systems (HMIS), Behavioural Factors, Community Health Promoters, Community Based Health Management Information Systems
1. Introduction
The focus for many health stakeholders has been to improve health outcomes. Achieving this entails having focus areas, one of which is health systems strengthening (HSS)
. Globally, health management information systems (HMIS) as a pillar of health systems have gained recognition due to potential of technology to strengthen health systems and improve access to quality care in underserved communities
. In sub-Saharan Africa (SSA), the new paradigm shift in strengthening health systems has increased the use of technology in healthcare at the community level, such as Community Based Health Information Systems (CBHIS), is becoming increasingly important for improving health outcomes and decision-making processes. This approach has gained much fame and preference over disease-specific health responses in formulation of health agendas both globally and nationally
| [9] | Kihara, P. (2016). Strategy Implementation and Performance of Manufacturing Firms in Kenya. Latvia, European Union: Lap Lambert Academic Publishing. |
[9]
. The global consensus is that a systems approach is required to ameliorate the present status of population health outcomes. A health system as defined by WHO
entails “all the organizations, institutions, resources and people whose primary purpose is to improve health.”An effective health system has six key pillars which are interrelated and work together to achieve the goals of a health system
| [19] | Ministry of Health (2016). Kenya Master Health Facility List: Find all the health facilities in Kenya. Retrieved November 4, 2016, from http://kmhfl.health.go.ke/#/home |
[19]
. These pillars include service delivery, health workforce, information, medical products (including vaccines and technologies), health care financing, leadership and governance
. A Community based Health Management Information System (CbHMIS) is used by community health extension workers (CHEWs) at the household level. It helps them plan, organize and keep track of their work with families including education and provision of healthcare services
| [9] | Kihara, P. (2016). Strategy Implementation and Performance of Manufacturing Firms in Kenya. Latvia, European Union: Lap Lambert Academic Publishing. |
[9]
.
Worldwide, there has been the need to strengthen health information and information constituencies. Community units are key players in extended healthcare systems reason being that they dispense services yet they do not form the officially recognized structure of health ministries
. They majorly serve the marginalized, providing them with their basic healthcare needs. Rather than assuming a normative approach, they gather primary information from the people that is aligned with their objectives
. Since such data is more informative on the actual situation, donors’ make use of it to review their funding needs
| [16] | Mbondenyi & Ambani (2014) The New Constitutional Law of Kenya. Principles, Government and Human Rights: Principles, Government and Human Rights. |
[16]
. In Brazil, a decentralized approach using paid health agents (HAs) has been shown that it could improve access to health care, however, its CbHMIS use component still undefined
. Thailand’s community involvement in health brought collaboration between government and non-government organizations, the empowerment of communities have been realized, however, the component of CbHMIS is still not given the attention it requires
.
There has been great emphasis from National governments and donors to support the work of CHPs towards universal health care expansion and coverage
| [12] | Mambo, S. N, Odhiambo-Otieno G. W, Ochieng’ Otieno G. and Wanja Mwaura T. (2018). Improving Health Systems: Influence of Technical Capacities of Community Health Volunteers on Use of Community Health Information Systems in Kenya. International Journal of Computer Applications (0975 – 8887) Volume 181 – No. 3, July 2018. |
[12]
. CHPs have gained worldwide recognition in global health policies as depicted in their adoption in USAID's policy for ending preventable child and maternal deaths (EPCMD) and President Uhuru’s Malaria Initiative that is a step towards achieving his universal healthcare agenda
| [6] | Jeremie N., Kaseje, D., Olayo, R., & Akinyi, C. (2014). Utilization of Community-based Health Information Systems in Decision Making and Health Action in Nyalenda, Kisumu County, Kenya. Universal Journal of Medical Science, 2(4), 37–42. |
[6]
. At the lower level, CHPs are important in narrowing down policies to the extent that they are applicable in community-based programs, especially in poverty-stricken and marginalized areas. Applicability of such initiatives at community level is bound to equity in healthcare
| [11] | Mambo, S. N, Odhiambo-Otieno G. W, Ochieng’ Otieno G. and Wanja Mwaura T. (2021). Health systems strengthening: assessing the influence of organizational factors of community health volunteers on use of community based health information systems in selected counties, Kenya. International journal of community medicine and public health. |
[11]
. However, there is no information on the global application of CBHIS
| [12] | Mambo, S. N, Odhiambo-Otieno G. W, Ochieng’ Otieno G. and Wanja Mwaura T. (2018). Improving Health Systems: Influence of Technical Capacities of Community Health Volunteers on Use of Community Health Information Systems in Kenya. International Journal of Computer Applications (0975 – 8887) Volume 181 – No. 3, July 2018. |
[12]
.
In Sub Saharan Africa, there is the recognition of the importance of health information systems to be capable of generating reliable data and information
| [19] | Ministry of Health (2016). Kenya Master Health Facility List: Find all the health facilities in Kenya. Retrieved November 4, 2016, from http://kmhfl.health.go.ke/#/home |
[19]
. Although there has been a concurrent increase in the production of data in the health sector, there has been little corresponding change in the use of such data to improve health care
. In Ethiopia CbHMIS implementation in the year 2010 gave a positive outcome in change in community level health management
. In Ethiopia there exists a Monitoring and Evaluation (M&E) system in which data is transmitted from the community units to the health Center. However there are no data collection tools and the CHEWs use note books to collect data
. In Malawi, Community Health Promoters exists, however, they do not have clearly defined roles and they are engaged by the Health Service Assistants whenever they require their support
.
CbHMIS has been applied in Ethiopia in the Southern Nations, Nationalities and Peoples’ Region (SNNPR). The project commenced in October 2010 and took two years. The region has seen a lot of improvement since then in the healthcare sector for instance service provision to children and pregnant women using the tickler file system as well as the use of collected information for planning in the region
| [16] | Mbondenyi & Ambani (2014) The New Constitutional Law of Kenya. Principles, Government and Human Rights: Principles, Government and Human Rights. |
[16]
. The success its implementation may be attributed to the region’s committed and respected leaders, the organizational ability of the community as well as partnership with others
.
Health sector reform and decentralization have brought about shifts in functions between the central and peripheral levels and have generated new information needs with changing requirements for data collection, processing, analysis and information dissemination
| [19] | Ministry of Health (2016). Kenya Master Health Facility List: Find all the health facilities in Kenya. Retrieved November 4, 2016, from http://kmhfl.health.go.ke/#/home |
[19]
. A study on Health systems Strengthening (HSS) in Zimbabwe revealed that policy implementation led to the magnification of health barriers rather than breaking them down
| [13] | Mambo, S. N, Odhiambo-Otieno G. W, Ochieng’ Otieno G. and Wanja Mwaura T. (2018). Assessing the influence of process interventions of community health volunteers on use of Community Based Health Management Information Systems in selected Counties, Kenya. http://www.ijsrp.org/research-journal-0818.php |
[13]
. (Lehmann & Matwa, 2008). This study showed that health policy implementation in its self is not a solution to health services if the health policies are not based on empirical data that aids in generating information for decision making
| [11] | Mambo, S. N, Odhiambo-Otieno G. W, Ochieng’ Otieno G. and Wanja Mwaura T. (2021). Health systems strengthening: assessing the influence of organizational factors of community health volunteers on use of community based health information systems in selected counties, Kenya. International journal of community medicine and public health. |
[11]
.
In Kenya, there are diverse examples from the literature of instances where community data are routinely collected and documented to influence change. For example, in Kisumu County, Kenya, CHEWs and CHPs were trained to facilitate community dialogue and maintain the CbHMIS and the village register. Health status data from each household were routinely collected and maintained by CHPs through the village register, and then analyzed by community members and committees and at the health center. Data-driven participatory action planning by the community and health centers helped to improve services. Reports are sent to the district-level, where they were processed electronically
| [12] | Mambo, S. N, Odhiambo-Otieno G. W, Ochieng’ Otieno G. and Wanja Mwaura T. (2018). Improving Health Systems: Influence of Technical Capacities of Community Health Volunteers on Use of Community Health Information Systems in Kenya. International Journal of Computer Applications (0975 – 8887) Volume 181 – No. 3, July 2018. |
[12]
.
The Counties saw statistically significant improvements in immunization coverage, health-facility childbirth, use of insecticide-treated bed-nets, and treated drinking water in comparison with control sites. In another example, under the Kenya Essential Health Package, CHEWs informed community health committees on key community health indicators, whereupon data collection was planned
| [6] | Jeremie N., Kaseje, D., Olayo, R., & Akinyi, C. (2014). Utilization of Community-based Health Information Systems in Decision Making and Health Action in Nyalenda, Kisumu County, Kenya. Universal Journal of Medical Science, 2(4), 37–42. |
[6]
. Data collected are then fed back to the facility to identify health utilization gaps and outbreaks, and ultimately to improve services.
The framework, called the Performance of Routine Information System Management (PRISM), identifies behavioral factors as one of the components necessary to improve routine information systems and the use of the data they generate
| [1] | Aqil, A., Lippeveld, T., & Hozumi, D. (2009). PRISM framework: A paradigm shift for designing, strengthening and evaluating routine health information systems. Health Policy and Planning, 24(3), 217–228. https://doi.org/10.1093/heapol/czp010 |
[1]
. Behavioral factors have been taken by similar researchers to refers to personnel Attitudes, Value of information, personnel perceptions and personnel motivation
.
This component refers to the behaviors of data users and how data are used to generate information for problem solving and program improvement at all levels of health care delivery
| [1] | Aqil, A., Lippeveld, T., & Hozumi, D. (2009). PRISM framework: A paradigm shift for designing, strengthening and evaluating routine health information systems. Health Policy and Planning, 24(3), 217–228. https://doi.org/10.1093/heapol/czp010 |
[1]
. Programmes that empower communities are likely to be acceptable since communities participate in guiding them. According to Odhiambo-Odhiambo 2007, this translates to the amount and details recorded depended on programme objectives, data and information use, the understanding of the message to pass across and literacy of the CHPs
| [23] | Nzinga, J., Mbaabu, L., & English, M. (2013). Service delivery in Kenyan district hospitals–what can we learn from literature on mid-level managers? Human Resources for Health, 11(1), 1. |
[23]
. Consequently, evidence from implementation of community strategy in Nyanza good health status primarily depended on factors beyond the health sector. Well-coordinated actions across sectors at the community level would increase efficiency in improving health outcomes
| [6] | Jeremie N., Kaseje, D., Olayo, R., & Akinyi, C. (2014). Utilization of Community-based Health Information Systems in Decision Making and Health Action in Nyalenda, Kisumu County, Kenya. Universal Journal of Medical Science, 2(4), 37–42. |
| [14] | Measure Evaluation (2009). Technical Consultation on Information Systems for Community-Based HIV Programs: MEASURE Evaluation. Retrieved August 30, 2017, from https://www.measureevaluation.org/our-work/hiv-aids/community-based-hiv-info-systems/hiv-meeting-registration/folder_contents?show_all=true |
[6, 14]
.
When dealing with communities in HMIS promotion, the aspect of attitude in behavior change is imperative. Pepela and Odhiambo-Otieno in their work noted that CHPs engagement was expected to diffuse community change to individuals
| [24] | Odhiambo-Otieno, G. W., & Odero, W. W. (2005). Evaluation criteria for the district health management information systems: Lessons from the Ministry of Health, Kenya. African Health Sciences, 5(1), 59–64. |
[24]
. In addition, they were expected to reduce disparities through improving access to care, providing culturally competent health education, counseling, and sometimes rendering direct health services. Also as trusted members of the community would additionally sensitize members of families to minimize barriers to health care resulted from health beliefs and health values
| [24] | Odhiambo-Otieno, G. W., & Odero, W. W. (2005). Evaluation criteria for the district health management information systems: Lessons from the Ministry of Health, Kenya. African Health Sciences, 5(1), 59–64. |
[24]
.
In another article, more than 350 participants “Celebrating 20 years of improving health in Kenya” marked PATH’s work over two decades to address critical health needs of improving health services, strengthening community networks, and empowering Kenyans to adopt healthier lifestyles
. The communities had their own social networks and information sharing platforms that included the forums that would be either formal or informal. This attracted negotiation tables to build in mechanisms to self-sustaining projects with elaborated communication and linkages
| [9] | Kihara, P. (2016). Strategy Implementation and Performance of Manufacturing Firms in Kenya. Latvia, European Union: Lap Lambert Academic Publishing. |
[9]
.
1.2. Value of Information
Communities can be empowered by helping them produce good information and its value cannot be overemphasized
| [11] | Mambo, S. N, Odhiambo-Otieno G. W, Ochieng’ Otieno G. and Wanja Mwaura T. (2021). Health systems strengthening: assessing the influence of organizational factors of community health volunteers on use of community based health information systems in selected counties, Kenya. International journal of community medicine and public health. |
[11]
. The implementation of the community health strategy necessitates the collection of data at community level to provide material for discussion during the community health committee meetings, which in term informs the actions of the ministry of health in regards to addressing the needs of the specified community
| [6] | Jeremie N., Kaseje, D., Olayo, R., & Akinyi, C. (2014). Utilization of Community-based Health Information Systems in Decision Making and Health Action in Nyalenda, Kisumu County, Kenya. Universal Journal of Medical Science, 2(4), 37–42. |
| [22] | Nutley, T. (2012). Improving Data Use in Decision Making: An Intervention to Strengthen Health Systems: MEASURE Evaluation. Retrieved November 4, 2016, from https://www.measureevaluation.org/resources/publications/sr-12-73 |
[6, 22]
.
In a study of providing evidence on programmes, activities, costs and impact on health outcomes of using community health workers stated that CHPs would make a valuable contribution to community development and, more specifically, improved access to and coverage of communities with basic health services
. They also showed that, there was robust evidence that CHPs would undertake actions that led to improved health outcomes especially, but not exclusively, in the field of child health
| [23] | Nzinga, J., Mbaabu, L., & English, M. (2013). Service delivery in Kenyan district hospitals–what can we learn from literature on mid-level managers? Human Resources for Health, 11(1), 1. |
[23]
. However, although they would implement effective interventions, they did not consistently provide services likely to have substantial health impact and the quality of services they provided was sometimes poor
| [16] | Mbondenyi & Ambani (2014) The New Constitutional Law of Kenya. Principles, Government and Human Rights: Principles, Government and Human Rights. |
| [13] | Mambo, S. N, Odhiambo-Otieno G. W, Ochieng’ Otieno G. and Wanja Mwaura T. (2018). Assessing the influence of process interventions of community health volunteers on use of Community Based Health Management Information Systems in selected Counties, Kenya. http://www.ijsrp.org/research-journal-0818.php |
[16, 13]
.
Evidence report from studies done in South Africa, tried to establish the outcomes of Community Health Worker Interventions that had improved livelihoods of communities and reduced childhood illnesses and reduced mortality through community participation and leaderships of their activities
| [9] | Kihara, P. (2016). Strategy Implementation and Performance of Manufacturing Firms in Kenya. Latvia, European Union: Lap Lambert Academic Publishing. |
[9]
. The emphasis of the researchers was on the fact that when communities received information relation to their health, they tended to work towards improving the situation. This element suggested that information sharing at community level was one of the high value components of any sustainability strategy deployed for community health management
. What seemed to come out on the contrary was the perception that community involvement in health matters depended on actions elsewhere, such as actions identified and implemented by government
| [12] | Mambo, S. N, Odhiambo-Otieno G. W, Ochieng’ Otieno G. and Wanja Mwaura T. (2018). Improving Health Systems: Influence of Technical Capacities of Community Health Volunteers on Use of Community Health Information Systems in Kenya. International Journal of Computer Applications (0975 – 8887) Volume 181 – No. 3, July 2018. |
[12]
(Vujicic, Ohiri, & Sparkes, 2009).
Failing to include community members in decision making alienated them from the health programs and fewer people volunteered to be part of the health system as well to give information on the state of community health indicators. The community’s contribution to these projects had been primarily through the sacrifice and volunteerism of CHPs who compiled and continually updated the data sets. Lack of recognition and participation of health management teams in community dialoguing had contributed to unclear steps in addressing their health needs. It also changed the way people received, processed, and evaluated community health information. These attributes were also used to assist in the assessment of the community information system in Bungoma County and the factors affecting use of community health information to improve health outcomes (Odhiambo-Otieno & Odero, 2005).
To address health disparities involvement of the community, specifically the involvement of community health workers (CHPs) vary from making them an integral part of the care delivery team to involving them as community navigators, education providers, or outreach agents and inclusive in terms of administrative areas as well as interested groups. The lack of reporting on intervention costs and cost-effectiveness according to standardized and commonly accepted measures made it challenging to compare economic outcomes across CHPs intervention studies. It also made it even more complicated to compare cost-effectiveness between CHPs interventions and non- CHPs health care interventions currently being reported. Kihara, P.
| [9] | Kihara, P. (2016). Strategy Implementation and Performance of Manufacturing Firms in Kenya. Latvia, European Union: Lap Lambert Academic Publishing. |
[9]
, 2008 outlined that for CHPs to be able to make an effective contribution, they must be carefully selected, appropriately trained and very important adequately and continuously supported. Large-scale CHPs systems required substantial increases in support for training, management, supervision and logistics
| [23] | Nzinga, J., Mbaabu, L., & English, M. (2013). Service delivery in Kenyan district hospitals–what can we learn from literature on mid-level managers? Human Resources for Health, 11(1), 1. |
[23]
.
AMREF Health Africa in its 30 years of evaluation of Efficacy of Community-Based Health Care in Kenya, Kibwezi attempted to document the historical evolution of interventions, assessed AMREF’s programmes in relation to national health policy, analyzed successes of the various interventions in terms of project objectives, implementation processes, expected outputs and outcomes, achievements of partnerships and sustainability and identified programme challenges and lessons learnt that stakeholders participation in community interventions were key in programme success and shared responsibilities
| [19] | Ministry of Health (2016). Kenya Master Health Facility List: Find all the health facilities in Kenya. Retrieved November 4, 2016, from http://kmhfl.health.go.ke/#/home |
[19]
. The evaluation, moreover, did not give the negative factors associated with implementation of the project but concentrated more on successes
.
1.3. Personnel Perceptions
Personnel perceptions have an impact on the adoption and use of CbHMIS. The perception of personnel of non-usefulness of information collection at lower levels of the health system leaders to lowering of the commitment of the health providers
| [13] | Mambo, S. N, Odhiambo-Otieno G. W, Ochieng’ Otieno G. and Wanja Mwaura T. (2018). Assessing the influence of process interventions of community health volunteers on use of Community Based Health Management Information Systems in selected Counties, Kenya. http://www.ijsrp.org/research-journal-0818.php |
[13]
.. This essentially indicates that if those who are involved in collecting primary data while offering health care find out that those who need the information don’t value it, their perception of the process is damaged, and hence they show lower levels of commitment.
At the service delivery level, the adoption of Community based health information systems was found to have a neutral effect on health workers perceptions that patient care improved as a result of the system
| [12] | Mambo, S. N, Odhiambo-Otieno G. W, Ochieng’ Otieno G. and Wanja Mwaura T. (2018). Improving Health Systems: Influence of Technical Capacities of Community Health Volunteers on Use of Community Health Information Systems in Kenya. International Journal of Computer Applications (0975 – 8887) Volume 181 – No. 3, July 2018. |
[12]
. This indicates that the adoption of a CbHMIS is not a sure fire way of the improving the perception of health workers towards the usefulness of the systems. Personnel perceptions of the effectiveness of health information systems were also shaped by patient perceptions of improvements in service delivery
| [11] | Mambo, S. N, Odhiambo-Otieno G. W, Ochieng’ Otieno G. and Wanja Mwaura T. (2021). Health systems strengthening: assessing the influence of organizational factors of community health volunteers on use of community based health information systems in selected counties, Kenya. International journal of community medicine and public health. |
[11]
. If the health workers don’t sense an increase in the confidence of patients after the deployment of a CbHMIS, they are likely to have poor perceptions of its usefulness.
1.4. Personnel Motivation
The ministry of Health in Malaysia launched a program in 2013 that was called
Komuniti Sihat, Perkasa Negara (KOSPEN) which in English meant that a strong community is the foundation of a strong nation
| [4] | Gilson, L., Daire, J., Patharath, A., & English, R. (2011). Leadership and governance within the South African health system. Durban: Health Systems Trust. |
[4]
. The program intended to transform how Malaysia approached its public healthcare strategy and it sought to recruit volunteers to serve as agents in the programs as one of its components
| [4] | Gilson, L., Daire, J., Patharath, A., & English, R. (2011). Leadership and governance within the South African health system. Durban: Health Systems Trust. |
[4]
.
Chung et al. (2017) in their study divided motivation into (extrinsic and intrinsic motivator, financial, skill, and performances). For extrinsic motivation factors, the data showed that prestige and respect factors motivated the respondents to perform 2.76 times better than those who were not (95% CI = 1.244, 6.120). Recognition as “doctor” in the community also motivated them to continue performing better as high as 8.65 times as compared to those who do not agree to this (95% CI = 2.044, 36.577). In addition, sufficient supplies of job aids such as boots, raincoat, and medical equipment influenced the respondents at 8.65 times higher performance as compared to those who do not think job aids can influence their work (95% CI = 1.324, 7.008). The respondents also revealed that the training location is important to affect their services especially those trainings carried out in community setting which have 4.76 times higher performance than those in government setting (95% CI = 1.930, 11.725). In this study, the community members/leaders played a more effective role than medically trained personnels in field supervision of CHV (OR = 7.15, 95% CI = 2.832, 18.055)
| [4] | Gilson, L., Daire, J., Patharath, A., & English, R. (2011). Leadership and governance within the South African health system. Durban: Health Systems Trust. |
[4]
.
Viswanathan et al. (2009) conducted 53 studies on characteristics and outcomes of CHPs interventions. They emphasized that through continuous community involvement and participation, CHPs were motivated to address their own health needs and cultivated knowledge sharing among the community members. This would promote sustainability mechanisms in improving their own health. However, the concept of community ownership and participation was often ill-conceived and poorly understood as a by-product of programmes initiated from the centre as stated by
| [6] | Jeremie N., Kaseje, D., Olayo, R., & Akinyi, C. (2014). Utilization of Community-based Health Information Systems in Decision Making and Health Action in Nyalenda, Kisumu County, Kenya. Universal Journal of Medical Science, 2(4), 37–42. |
[6]
.
In a study on utilization of Community-based Health Information Systems in Decision Making and Health Action in Kisumu stated that the experiences of their two study sites demonstrate these facts; the initial challenge already could be seen in ensuring that the CHPs are well trained; CHPs respondents mentioned these frequently as one way of motivating to gain confidence in their work; it is also seen that the sources of information are many and varied which requires continued updates and refresher training so that the CHPs are skilled in gathering these information and collating them
| [6] | Jeremie N., Kaseje, D., Olayo, R., & Akinyi, C. (2014). Utilization of Community-based Health Information Systems in Decision Making and Health Action in Nyalenda, Kisumu County, Kenya. Universal Journal of Medical Science, 2(4), 37–42. |
[6]
. This coincides with a 2012 assessment of how quality of data can be enhanced in Zanzibar, information about health challenges in the community; the data-use workshops with active engagement of data users themselves as a unique active way of improving health information systems overall and enhance staff capacity and motivation for information use, presentation and analysis for decision-making
| [13] | Mambo, S. N, Odhiambo-Otieno G. W, Ochieng’ Otieno G. and Wanja Mwaura T. (2018). Assessing the influence of process interventions of community health volunteers on use of Community Based Health Management Information Systems in selected Counties, Kenya. http://www.ijsrp.org/research-journal-0818.php |
[13]
.
Pepela and Odhiambo-Otieno (2016) in their study in Bungoma emphasized that Programmes that empowered communities were likely to be acceptable since communities participated in guiding them. The amount and details recorded depended on programme objectives, data and information use, the understanding of the message to pass across and literacy of the CHPs. Consequently, evidence from implementation of community strategy in Nyanza
| [6] | Jeremie N., Kaseje, D., Olayo, R., & Akinyi, C. (2014). Utilization of Community-based Health Information Systems in Decision Making and Health Action in Nyalenda, Kisumu County, Kenya. Universal Journal of Medical Science, 2(4), 37–42. |
[6]
good health status primarily depended on factors beyond the health sector. Well-coordinated actions across sectors at the community level would increase efficiency in improving health outcomes. Individuals were responsible for the day- today up keep of the household affairs as well as participated in community organized activities and this formed the first level of care that was universally available. This had been domesticated with a theme by the community health workers as “AfyaYetu, Jukumu Letu”. This included nurturing communities to economic empowerment, transformation, enhanced access to the means of production, marketing and payed attention to the social determinants of health.
It could also be argued that all these sectors and actors would be represented on the Community Health Committee to the extent possible. This was also supported by Odhiambo-Otieno and Odero (2005) in their article that Village Health Committees (VHCs) members were decided by the village members and Health Centre Development Committee (HCDC) was made up of representative chairpersons of VHCs in the facility's catchment area, and was chaired by one of them
| [24] | Odhiambo-Otieno, G. W., & Odero, W. W. (2005). Evaluation criteria for the district health management information systems: Lessons from the Ministry of Health, Kenya. African Health Sciences, 5(1), 59–64. |
[24]
.
In Kenya, according to a situation analysis on the state of Community Health Services in year 2014, the functionality of CbHMIS was said to be at 64% and has been recording a drop to currently at 55% in year 2016, and that access to quality data was not guaranteed through the current CbHMIS (
, Kaburi, & Okero, 2016). Some known and assumed barriers to the CbHMIS use include: lack of physical access, lack of awareness of what is available; lack of relevance of available information (not meeting peoples' needs in terms of scope, style or format); lack of time and incentives to access information; and lack of interpretation skills (Flora, Margaret, & Dan, 2017). Due to poor understanding, under-resourcing and undermanaging of community based information systems and services, these problems continue to be elated
| [6] | Jeremie N., Kaseje, D., Olayo, R., & Akinyi, C. (2014). Utilization of Community-based Health Information Systems in Decision Making and Health Action in Nyalenda, Kisumu County, Kenya. Universal Journal of Medical Science, 2(4), 37–42. |
[6]
.
Behavioral factors of CHPs influence to great extent the CbHMIS use. The major factor under this is motivation of the CHPs which is always seen as an enabler of their services but in many instances it is never forthcoming. Many counties have not factored financial motivation of CHPs in their budgets and hence the volunteers do not pay much attention to their work. Community-based programmes and CHPs are intertwined such that achieving success of one requires the success of the other. A tool to promote such success is motivation of CHPs. It gives them the drive and ambition to provide the desired results. Hypothesis: The study set out to proof the following hypothesis.
H02: Behavioral factor of Community Health Promoters does not influence the use of Community based Health Management Information Systems in Kenya.
H2: Behavioral factor of Community Health Promoters significantly influences the use of Community based Health Management Information Systems in Kenya.
2. Methods
Mixed method cross sectional study design was utilized, which employed both quantitative, qualitative, and descriptive approaches. Study areas encompassed three selected counties; Kiambu categorized as a peri-urban county, Kajiado categorized as a rural county and Nairobi categorized as an urban County.
The study population for this study was 156 active CU’s from the three selected counties where a sample of 122CUs was drawn. Three (3) CHPs from each community unit were interviewed. Focus Group Discussion were done on 3 Functional community health committees (CHCs), one from each county. Six Key informants (CHEWs (PHO’s) and County Coordinator) were considered with two from each county. Only CHPs who had been trained using the community strategy curriculum and have been on operation for at least one year in the selected counties were selected.
Sample Size Determination (Quantitative data)
The following general standards of sample size determination for the health sciences were used to identify the sample size for the proposed study:
Alpha-level of significance (probability level) is set at 0.05 which means the confidence level was set at 95% (5% chance of making type I error or false positive result);
Power of statistical test (1-β) was set at 0.80 which means 20% chance of making type II error or false negative result;
Effect size range was set between 0.20 to 0.40 (measure of the strength of the relationship between two variables) (Alreck & Settle, 2004; Raosoft, 2004).
The study sample was then selected using the formulae given by Mugenda and Mugenda (2003) where the sample size for a population of 10,000 or more is computed using the formula given below:
Where, n = Minimum Sample Size p = Population proportion with given characteristic z = Standard normal deviation at the required confidence level
e = Error Margin. Mugenda and Mugenda recommend that since p and q are unknown, both are set at 50%. At a confidence level of 95% that was used for this study, z = 1.96 and the sampling error of e = +5%. Thus, sample size n becomes:
N = 50*50*(1.96/5) 2 = 384
For a population less than 10,000, the sample is computed as follows;
Where, nf = desired sample size when the population is less than 10,000
Using this formula, a sample size of 366 CHPs were selected for the purpose of this study. A sample of 122CUs were be drawn from 156 active CUs.
The population of the active (Fully Functional) Community units is given as N =156 then the sample size n = 384.
The first step involved selection of a representative sample size. The total population (156)
| [20] | Mugenda, O., & Mugenda, A. (2003). Research Methods: Quantitative and Qualitative Approaches. Nairobi: ACTS. |
[20]
recommendations for quantitative sampling.
Sample for the Community Units (CUs)
Fully functional CUs=156
= 111 CUs (10% attrition rate (11))
An attrition rate of 10% was considered. Attrition is the loss of randomly assigned participants or participants’ data, which can bias a randomized controlled trial's external validity by producing a final sample that is not representative of the population sampled, or, if differential between study arms, can result in some characteristic of the retained sample causing an observed intervention effect
| [20] | Mugenda, O., & Mugenda, A. (2003). Research Methods: Quantitative and Qualitative Approaches. Nairobi: ACTS. |
[20]
.
Using this formula, a sample of 122 CUs were selected randomly and 3 Community Health Promoters were interviewed from each CU which formed a total sample of 366 CHPs as respondents for this study. Multi stage sampling was used to arrive at a desired sample size. Systematic sampling was used to identify the Community Units and purposive sampling was used to sample the three respondents per Community Unit as shown in
Table 1.Table 1. Sample size determination.
County | Est CUs | Fully Functional (FF) CUs | Sample calculation for CUs | Total CUs per County | Sample calculation for Respondents (CHPs) | Respondents CHPs Per CU (Purposive sampling) |
Kiambu | 79 | 64 | nf = /(1+n/N) = 384/1+ (384/156) = 384/3.462 = 110.933 = 111 CUs (10%) attrition rate (11) = 122 CUs | (64/156)* 122= 50 | nf = /(1+n/N) N= 156*50 =384/1+ (384/7800) = 384/1.05 = 365.7 = 366 | 50*3=150 |
Kajiado | 56 | 33 | | (33/156)*122=26 | | 26*3=78 |
Nairobi | 140 | 59 | | (59/156)*122=46 | | 46*3=138 |
Total | 275 | Target Population 156 CUs | | 122 CUs | | 366 CHPs (Respondents) |
Sample Size Determination (Qualitative Data)
Qualitative data was collected through focus group discussions (FGD) and key informant interviews (KIIS). 3 FGDs were conducted, 1 from each county (with the CHC’s). A total of 6 KII, 2 from each county were conducted (1County Community strategy coordinator; and one Sub county community strategy focal person (CHEW).
Document review was done to inform literature review. Quantitative data was collected using an interviewer administered questionnaire administered to all sampled CHPs, supplemented voice recording of specific interviews and also focus group discussions and note taking during these processes. Qualitative data was collected through focus group discussions and Key Informant interviews. The Community Health Committees formed respondents for the FGDs while CHEWs and County Coordinators were the Key Informants that helped elaborate on the reasons of use and disuse, usage patterns and to validate findings made via quantitative methods.
Quantitative Data was analyzed using computer based software, with preference being the SPSS version 23 package of data analysis. The key analysis done in this study were: Test of normality of the data, test of hypothesis, significance test of variables through use of P values P<.005 level of significance; Chronch bach Alpha was also utilized to test reliability; F-test statistics was considered as a measure of model validity and Pearson (r) for bivariate correlation analysis. Results were presented in form of tables, figures and narration.
Qualitative data was analyzed using manual content analysis based on key themes generated from objectives. Some Key themes were reported as said by the key informants. Multiple manual coding was done to create coding categories which were capable of reflecting the content of the data. The coding categories extracted from the transcripts were used to systematically analyze commonalities and apparent perceptions reflected in the data by focusing on issues which were repeatedly mentioned or strongly emphasized by the informants. Responses were compared across the region of respondents (CHCs – Kiambu, Kajiado Nairobi).
This Study Utilized Different Tests for Hypotheses
Table 2. Test of hypothesis.
Variable | Null Hypothesis | Type of Analysis | Interpretation |
Behavioral factors | H02 No significant difference | Pearson Correlation Linear Regression | P < 0.05 reject null P > 0.05 fail to reject null |
Ethical clearance to conduct the research was obtained from Kenya Methodist University Science, Ethics and Research Committee (SERC) Letter of permission was also obtained from National Council for Science and Technology (NACOSTI) as well as from the Counties of focus that is Kiambu, Kajiado and Nairobi County Health Office. Protocol was also ensured in the field and permission from the county health management was sought. Informed consent was obtained from the study participants before interviews were conducted. The participants were not identified by name either in the questionnaire or during data reporting to ensure confidentiality. Interviews were conducted in a secluded place, which ensured privacy.
3. Results
This study was geared towards establishing whether behavioral factors of Community Health Promoters influence use of Community based Health Management Information Systems in Kenya; This was measured using the following behavioural factors indicators: Attitudes, Motivation, Values and perceptions: All the 366 questionnaires used to interview the respondents were complete and fit for data analysis. This gave a 100% response rate for the study.
3.1. Demographic Characteristics of the Respondents
The findings show that majority of CHPs in the Community Units are in their middle ages hence relatively young. Since the younger CHPs have relatively low engagements in the community and less parental roles, serving the communities at voluntary basis is easier for them. Female respondents accounted for 73% of the entire sample while male respondents accounted for only 27%. This implies that Community Units in Kenya is largely dominated by females in terms of gender. Findings indicated that majority of the CHPs have attained secondary level education 43%, followed by 38% who have attained primary level education which is the minimum CHV entry level and very few respondents have attained University at only 2%. Majority of the respondents indicated that their monthly income is below 10,000KSh. 66%, and 17% of them were earning between 10,000 and 20,000 respectively monthly.
Information based on important demographic characteristics of the respondents were cross-tabulated. The results in this table are a cross-tabulation of the Gender, against education level and income of the respondents. The findings indicate that among the females who are earning below 10,000, 44.8% had attained primary level education, 38.3% had attained secondary education level, 16.4% had attained college level while only 0.5% had attained the University level. The observation here is that majority of the CHPs have only attained primary level education and hence this explains their low income level.
Among the male respondents, those earning below 10,000Ksh 41.1% had attained primary education, another 41.1% had attained secondary education and only 16.1% and 1.8% had attained college and University respectively. The general observation here is that the females who earned less than 10,000 and had only attained primary level education were more their male counterparts as indicated in
table 3.Table 3. Gender, Education and Income of Respondents: Cross-tabulation.
Gender * Education level * Income Cross-tabulation |
Income | Education level | Total |
| Primary level | Secondary level | College | University | |
Below 10000 | Gender | Female | Count | 82 | 70 | 30 | 1 | 183 |
| | | % within Gender | 44.8% | 38.3% | 16.4% | 0.5% | 100.0% |
| | | % of Total | 34.3% | 29.3% | 12.6% | 0.4% | 76.6% |
| | Male | Count | 23 | 23 | 9 | 1 | 56 |
| | | % within Gender | 41.1% | 41.1% | 16.1% | 1.8% | 100.0% |
| | | % of Total | 9.6% | 9.6% | 3.8% | 0.4% | 23.4% |
| Total | Count | 105 | 93 | 39 | 2 | 239 |
| | % within Gender | 43.9% | 38.9% | 16.3% | 0.8% | 100.0% |
| | % of Total | 43.9% | 38.9% | 16.3% | 0.8% | 100.0% |
Influence of Behavioral factors on CbHMIS use.
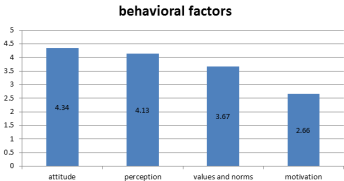
3.2. Descriptive Analysis on Behavioral Factor
Personnel attitudes; the respondents strongly agreed with that CHPs in the community units in Kenya love their job (composite mean score, 4.34), and that Volunteers are happy with their job (composite mean score, 4.08) Value of information respondents agreed with our Community unit strictly follows values and norms that guide their operations (composite mean score, 3.67). On personnel perceptions majority of the CHPs were in agreement that volunteers assist their clients satisfactorily and in a mature manner (composite mean score, 4.13), the households the respondents serve have positive perception on what they do (composite mean score, 4.00), that the households the CHPs serve are happy with their services (composite mean score, 4.06) and that Our clients easily welcome our volunteers (composite mean score, 3.89) as shown in
figure 1. Figure 1. Behavioral Factors.
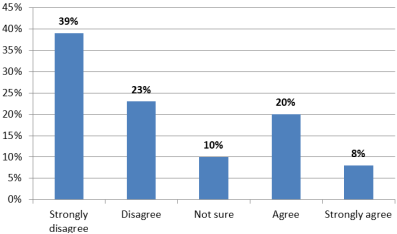
On personnel motivation, 39% of the respondents strongly disagreed that they are motivated to do their work while a 20% of them agreed on being motivated to do their work as shown by
figure 2. Figure 2. Motivation of CHPs to do their work.
Bivariate analysis: Relationship between behavioral factors and CbHMIS Use
The Bivariate correlations in
Table 4 showed a positive and significant influence of behavioral factors of Community Units personnel on the use of CbHMIS in Kenya (r =.366**,
P = .005). Amongst all the indicators investigated under behavioral factor, observation of values and norms in information use by CUs had the strongest association with the CbHMIS use (r =.304**,
P = .005). and perceptions of the CHPs towards their use of CbHMIS had the weakest association (r =.135**,
P = .005).
Table 4. Relationship between behavioral factor and CbHMIS use.
| Attitudes | Values | Perceptions | Beliefs | Motivation | Behavioral | CbHMIS use |
Attitudes of CU personnel | 1 | | | | | | |
| | | | | | | |
Values and Norms | .183** | 1 | | | | | |
| .000 | | | | | | |
Perceptions | .176** | .215** | 1 | | | | |
| .001 | .000 | | | | | |
Beliefs | .186** | .201** | .464** | 1 | | | |
| .000 | .000 | .000 | | | | |
Motivation | .117* | .349** | .131* | .064 | 1 | | |
| .026 | .000 | .012 | .222 | | | |
Behavioral factor | .474** | .666** | .597** | .545** | .692** | 1 | |
| .000 | .000 | .000 | .000 | .000 | | |
CbHMIS use | .171** | .304** | .135** | .248** | .233** | .363** | 1 |
| .001 | .000 | .010 | .000 | .000 | .000 | |
3.3. Dependent Variable: CbHMIS Use
The findings indicate that, most of the respondents are happy with having CHA/CHEW as their link person to the facility HMIS (composite mean score, 4.40), That the current health outcomes in the community are better informed by the decisions the CHPs have been making (composite mean score, 3.90), that the respondents make decisions regularly (composite mean score, 3.73), that most of the decisions are very timely (composite mean score, 3.52) and finally that the system is able to generate the information needed (composite mean score, 3.52).
However, the respondents disagreed with the following statements: that we make accurate decisions from the information we generate (composite mean score, 3.41), That we are able to use most of the information generated by our health management information system (composite mean score, 3.37), That we are always able to make quality decisions from the information we generate from the system (composite mean score, 3.35), and finally that I am able to access information from the computer management system when I need it (composite mean score, 2.58).
Table 5 shows CbHMIS items mean and SD.
Table 5. CbHMIS use indicators.
CbHMIS use constructs | n=366 |
| Mean | SD |
Our system is able to generate the information we need | 3.54 | 1.05 |
I am able to access information from the computer Management Information system when i need it | 2.60 | 1.25 |
We make accurate decisions from the information we generate | 3.42 | 1.12 |
We are able to use most of the information generated by our Health Management Information system | 3.38 | 1.20 |
We are happy with having CHEW as our link person to the facility HMIS | 4.41 | .77 |
The information we generate is always relevant | 3.94 | .89 |
We are always able to make quality decisions from the information we generate from the system | 3.36 | 1.07 |
The current health outcomes in our community are better informed by the decisions we have been making | 3.90 | .94 |
We make decisions regularly | 3.74 | 1.00 |
Most of our decisions are very timely | 3.52 | 1.14 |
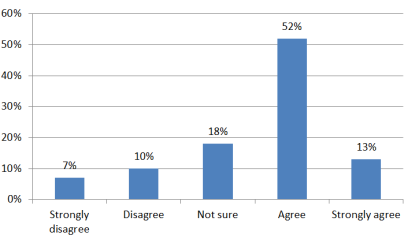
3.4. Information Reliability
Majority of the respondents 52% agrred that their system is able to generate the information they need while only 7% strongly disagreed as shown in
figure 3.
Figure 3. Accuracy of the system.
3.5. Respondents Level of Use of CbHMIS
Slightly above half of the participants interviewed reported that they were using the CbHMIS 56.6% (n=207) while those who reported non-use of the CbHMIS were 43.4% (n=159). A representation of use of CbHMIS is indicated in
Table 6.
During the FGD and Qualitative interviews, when asked about the level of use of CbHMIS by CUs, a respondent from an FGD said that”…We as the CHPs can actually say we are not adequately using the system because it is almost totally manual…. however our CHPs really want to use the system if enabled to do so it’s too manual that it does not enable us to effectively capture all the data we collect from the field, such that when we meet for dialogue days, we sometimes realize that some data is missing for a particular month from different CHPs which affects the accuracy of our information…”. A Key Informant from Kajiado on the same noted that “…our Community Health Promoters are very interested in using the system, I can actually say the use interms of reporting, interpreting and using it for dialogue days stands at approximately 45% which is very low …now this is compounded by availability of manual system which is currently at, 95% (the CHPs use forms to report and chalk boards to interpret their data currently which is not very effective) as opposed to only 5% which is electronic and has only been made possible by partners who are supporting only a very small number of our community units…”.
Table 6. Distribution of users of CbHMIS.
Use of CbHMIS | N=366 |
| n | % |
Non User | 159 | 43.4 |
User | 207 | 56.6 |
Total | 366 | 100.0 |
3.6. Influence of Behavioral Factor on CbHMIS Use
Emphasis on an attitude of taking responsibility and avoiding blame has been the key focus of behavior of the community health workers. The Bivariate correlations in
Table 7 indicated that there is a positive and significant influence of behavioral factors of Community Units personnel on the use of CbHMIS in Kenya (r =.373**,
P = .001). This implies that the use of CbHMIS by Community Units improves significantly when the CU personnel have better behavior.
Table 7. Relationship between CbHMIS use and independent variables.
| Y | X1 | X2 | X3 | X4 |
Use of CbHMIS (Y) | Pearson Correlation | 1 | | | | |
| Sig. (2-tailed) | | | | | |
| N | 365 | | | | |
Technical Capacity (X1) | Pearson Correlation | .560** | 1 | | | |
| Sig. (2-tailed) | .000 | | | | |
| N | 365 | 366 | | | |
Behavioral factors (X2) | Pearson Correlation | .373** | .364** | 1 | | |
| Sig. (2-tailed) | .000 | .000 | | | |
| N | 365 | 366 | 366 | | |
Organizational factors (X3) | Pearson Correlation | .632** | .436** | .422** | 1 | |
| Sig. (2-tailed) | .000 | .000 | .000 | | |
| N | 365 | 366 | 366 | 366 | |
Process Interventions (X4) | Pearson Correlation | .438** | .168** | .523** | .510** | 1 |
| Sig. (2-tailed) | .000 | .001 | .000 | .000 | |
| N | 365 | 366 | 366 | 366 | 366 |
*. Correlation is significant at the 0.05 level (2-tailed).
These findings were subjected to further analysis where a univariate linear regression model
Y = β0 + β2X2 + ε was used to determine the influence of behvioural factor on use of CbHMIS by CUs. Results in
Table 8 shows that the model is valid (F
(1, 363) = 58.579,
P =
.001) hence the explanatory variable (X
2, Behavioral factors) is good in explaining total variations in Use of CbHMIS by community units.
Table 8. Behavioral Factors and CbHMIS use: Model Validity.
Model | Sum of Squares | df | Mean Square | F | Sig. |
| Regression | 18.325 | 1 | 18.325 | 58.579 | .000b |
| Residual | 113.557 | 363 | .313 | | |
| Total | 131.882 | 364 | | | |
a. Dependent Variable: CbHMIS use (Y) |
b. Predictors: (Constant), Behavioral Factors (X2) |
The study further showed that the behavioral factors of Community Health Promoters (X
2)
explains 13.7% of the total variation in the use of information by community units in CbHMIS (R
2 = .137). The value of the constant in the
Table 9 shows that the behavioral factors of Community Health Promoters will always exist at a certain minimum (β
0 = 2.249,
P < .001). The behavioral factors of Community Health Promoters were found to influence the use of CbHMIS by community units positively and significantly (β
1= .359,
P < .001). This confirms the findings of the bivariate correlations in
Table 9 which indicated that when the behavioral factors of the CU personnel improve, the use of CbHMIS will also improve.
The univariate model in
Table 8 was found to be significant (P<0.001) and therefore, supports the mainobjective that the behavioral factors of community units personnel positively and significantly influences use of CbHMIS.
Table 9. Behavioral factors and CbHMIS use: Regression weights.
Model | Unstandardized Coefficients | Standardized Coefficients | R2 | t | Sig. |
| B | Std. Error | Beta | | | |
| (Constant) | 2.249 | .176 | | | 12.801 | .000 |
| Behavioral Factors (X2) | .359 | .047 | .373 | .137 | 7.654 | .000 |
a. Dependent Variable: (Use of CbHMIS (Y) |
Test of Hypothesis:
H02: Behavioral factor of CHV does not influence CbHMIS use in Kenya.
This hypothesis intended to test whether there is any influence between the behavioral factors and the use of CbHMIS. The hypothesis H0
2: β
1 = 0 versus H
2: β
1 ≠ 0 was tested. Results from the bivariate correlation in
Table 6 shows a significant and positive relationship between the behavioral capacity of community units personnel and use of CbHMIS (r =.373**, P = .001). On the other hand, the univariate regression results in
Table 7 also show that there is a positive and significant influence between behavioral factors of community units personnel and use of CbHMIS. (β
1=.359, P = .001). This leads to the rejection of the null hypothesis (H
01) and the acceptance of alternative hypothesis (H
1). The study, therefore, concludes that behavioral factors of community units personnel has a significant positive relationship influence on the use of CbHMIS in Kenya.
Community-based systems have the potential to make health services more inclusive and less discriminatory because they often work with marginalized groups. Similarly, community-based providers are “strategically placed to facilitate community participation and stimulate critical thinking; and third, they act as a catalyst to social action to address the social and cultural determinants of poor health. (Lenette, 2014).” Additionally, in a recent article by Sheikh, Ranson, & Gilson (2014), the authors argue that “health systems are also human systems” and as such “community norms and behaviour drive health market forces and practices, influence how individuals and families access services, and can help hold systems accountable.
The study findings showed that most of the Community Health Promoters (CHPs) in the community units have a positive feeling on the work they do in that they love their job as volunteers which has helped them achieve their objectives. These results agree with a study by Aqil that how an individual feels about the utility or outcomes of a task affects his/her confidence in performing that task, as well as the complexity of the task, all affect the likelihood of that task being performed
| [1] | Aqil, A., Lippeveld, T., & Hozumi, D. (2009). PRISM framework: A paradigm shift for designing, strengthening and evaluating routine health information systems. Health Policy and Planning, 24(3), 217–228. https://doi.org/10.1093/heapol/czp010 |
[1]
. Limited knowledge of the usefulness of RHIS data is found to be a major factor in low data quality and information use.
The findings indicated that the perception of both the Community Health Promoters and the households that they serve are very important in helping the community units generate the quality data that they require for informed decision making. This was indicated by the statements that the households the CHPs serve are happy with their services, the households the respondents serve have positive perception on what they do and that the clients easily welcome our volunteers.
Community unit strictly follows values and norms that guide their operations. Motivating CbHMIS users remain a big challenge as indicated by the findings of this study. This is despite the various trainings that the community units are offered. The findings of this study concur with a study by Aqil where he notes that motivation RHIS users remains a challenge despite training on data collection and data analysis. Negative attitudes such as ‘data collection is a useless activity or waste of care provider time’ hinder the performance of RHIS tasks
| [1] | Aqil, A., Lippeveld, T., & Hozumi, D. (2009). PRISM framework: A paradigm shift for designing, strengthening and evaluating routine health information systems. Health Policy and Planning, 24(3), 217–228. https://doi.org/10.1093/heapol/czp010 |
[1]
. Similarly, provision of material support including reporting tools and IEC materials to the community units by the counties which is supposed to be part of the motivation strategies was found to be very minimal and in some community units was not present at all.
Most of the CHPs view monetary motivation as the best by the mere fact that most of them are breadwinners, however, most of them work on volunteer basis and get very little if any remuneration from the partners who may engage them though for a very short while. There was a proposal to the Ministry of Health from the community strategy programme that indicated the government was to consider give a stipend of 2000 kshs to the Community health workers but it has not been honored despite the Community health workers views that it should be slightly more. They as Community Health Promoters argue that they use their own funds to assist community members in various ways for example going to other health facilities and in some severe cases buying food for the community members who are really poor in their respective community units.
In addition most Community Health Promoters choose to be involved in other activities so that they can get a source of livelihood. Studies from the united states of America (Kihara, 2016), enhance this fact further by showing a significant drop out of Community Health Promoters due to lack of career prospects and salaries. Therefore these are strong incentives in not only motivating and retaining Community health workers but also in enhancing their performance. Studies have also shown that Community Health Promoters with higher education qualifications have opportunities for alternative employment and therefore migrate from one job to another. This can be seen as a factor that is contributing to a large number of the Community Health Promoters working on part time basis
.
CbHMIS users’ cumulative behavior (attitude, values, perceptions and motivation to perform tasks) affect CbHMIS processes and performance directly as shown in
Table 10. This means it influences individual feelings on the utility and outcomes of an activity, or the confidence in task performance
| [24] | Odhiambo-Otieno, G. W., & Odero, W. W. (2005). Evaluation criteria for the district health management information systems: Lessons from the Ministry of Health, Kenya. African Health Sciences, 5(1), 59–64. |
[24]
.
Table 10. Summary of Results of Hypothesis Tested.
No. | Variable | P-Value | Direction | Deduction |
Hо2 | Behavioral factor | <.001 | Positive | Reject Hо2 |
4. Discussion
To Determine Effects of the Behavioral Factors of CU Personnel on CbHMIS Use in Kenya.
Behavioral factors in understanding CbHMIS factors in data users behavior, how data are analysed to generate information for evidence based problem solving and in the long run ensures program improvement at all levels of health care delivery (1). Programmes that empower communities are likely to be acceptable since communities participate in guiding them. According to Odhiambo-Odhiambo 2005, this translates to the amount and details recorded depended on programme objectives, data and information use, the understanding of the message to pass across and literacy of the CHPs
| [24] | Odhiambo-Otieno, G. W., & Odero, W. W. (2005). Evaluation criteria for the district health management information systems: Lessons from the Ministry of Health, Kenya. African Health Sciences, 5(1), 59–64. |
[24]
.
Pepela and Odhiambo-Otieno (2016) noted that CHPs engagement was expected to diffuse community change to individuals. In addition, they were expected to reduce disparities through improving access to care, providing culturally competent health education, counseling, and sometimes rendering direct health services.
A study on utilization of Community-based Health Information Systems in Decision Making and Health Action in Kisumu stated that the experiences of their two study sites demonstrate these facts; the initial challenge already could be seen in ensuring that the CHPs are well trained; CHPs respondents mentioned these frequently as one way of motivating to gain confidence in their work; it is also seen that the sources of information are many and varied which requires continued updates and refresher training so that the CHPs are skilled in gathering these information and collating them
| [6] | Jeremie N., Kaseje, D., Olayo, R., & Akinyi, C. (2014). Utilization of Community-based Health Information Systems in Decision Making and Health Action in Nyalenda, Kisumu County, Kenya. Universal Journal of Medical Science, 2(4), 37–42. |
[6]
.
This study found out that the behavioral factors of Community Health Promoters were influencing the use of CbHMIS by community units positively and significantly (β1= .359, P < .001). This confirmed all other related findings which indicated that when the behavioral factors of the CU personnel improve, the use of CbHMIS will also improve.
Generally, limited know-how of CbHMIS data usefulness is found to be a major factor in low data quality and information use. Most of the Community Health Promoters (CHPs) in the community units usually have a positive feeling on the work they do in that they love their job as volunteers which has helped them achieve their objectives. These results agree with a study by
| [1] | Aqil, A., Lippeveld, T., & Hozumi, D. (2009). PRISM framework: A paradigm shift for designing, strengthening and evaluating routine health information systems. Health Policy and Planning, 24(3), 217–228. https://doi.org/10.1093/heapol/czp010 |
[1]
. that how an individual feels about the utility or outcomes of a task affects his/her confidence in performing that task, as well as the complexity of the task, all affect the likelihood of that task being performed (1).
Motivating CbHMIS users remain a big challenge as indicated by the findings of this study. This is despite the various trainings that the community units are offered. The findings of this study concur with a study by Aqil
et al. (2009) where he notes that motivation RHIS users remains a challenge despite training on data collection and data analysis. Negative attitudes such as ‘data collection is a useless activity or waste of care provider time’ hinder the performance of RHIS tasks
| [1] | Aqil, A., Lippeveld, T., & Hozumi, D. (2009). PRISM framework: A paradigm shift for designing, strengthening and evaluating routine health information systems. Health Policy and Planning, 24(3), 217–228. https://doi.org/10.1093/heapol/czp010 |
[1]
.
Part of motivation strategies is provision of material support including reporting tools and IEC materials to the community units by the Counties, however, this was found to be very minimal and in some community units was not present at all. In return, this was noted to be very demoralizing.
Monetary motivation is still viewed as the best by most of the CHPs even though most of them are fully aware that they do work on voluntary basis. This is because most of them are breadwinners and therefore cannot afford to only volunteer as CHPs.
5. Conclusion
Behavioural factors are good in explaining total variations in Use of CbHMIS by community units. Limited knowledge of the usefulness of CbHMIS data is found to be a major factor in low data quality and information use. Motivation of Community Health Promoters (CbHMIS users) also remains unattended issue which greatly impacts on use of CbHMIS. This should be given in both monetary and non-monetary terms, for instance trainings and refresher training. Provision of material support including reporting tools and IEC materials to the community units by the counties can form part of the motivation strategies.
Generally the use of the CbHMIS system (both manual and electronic) in the selected counties is very low. The electronic system is almost non-existent in all selected counties. The low use is attributed to the system quality, individual and institutional factors discussed above. There is limited use of computers as equipment in the facility due to the limited number.
6. Recommendations
Behavioural factors highly affect use of CbHMIS, similarly limited knowledge of the usefulness of CbHMIS data is found to be a major factor in low data quality and information use this study therefore recommends, that the Community Health Promoters are equipped with more knowledge on CbHMIS that will help them change their negative attitude towards data collection and decision making at level one of service provision.
This study also recommends proper motivation of Community Health Promoters (CbHMIS users) because it’s a big challenge as indicated by the findings of this study. This should be given in both monetary and non-monetary terms, for instance trainings and refresher training). Provision of material support including reporting tools and IEC materials to the community units by the counties can form part of the motivation strategies.
What is already known on this topic:
1) Behavioural factors of CHPs in the community level health delivery is key
2) Community Health Promoters contribute greatly to a functioning of a health system
3) The overriding factor of any Pillars of a health system is the health inform pillar
What this study adds:
1) The results of this study contributes to achievement of national and international goals including the Sustainable Development Goals (SDGs) is becoming highly impossible without greater and more effective investment in health systems and service.
2) This study contributes to the body of knowledge on the influence of organizational factors on the use of CBHMIS and its of importance to scholars in academic and research institutions.
3) Similarly, the study has great importance to government and Counties, non-governmental organizations (NGO’s) in Kenya as a means of reviewing their own Community-based health management information systems.
Abbreviations
AMREF: African Medical Research Foundation Health Africa
CAD: Community Action Days
CbHMIS: Community-based Health Management Information System
CBO: Community Based Organization
CDD: Community Dialogue Days
CHC: Community Health Committee
CHEW: Community Health Extension Worker
CHW/V/P: Community Health Worker/Volunteer/Promoter
CU: Community Unit
DHMIS: District Health Management Information System
DHIS1: District Health Information System1
DHIS2: District Health Information System2
GAVI: Global Alliance on Vaccines and Immunization
GFTAM: Global Fund to Fight AIDS, TB, and Malaria
GoK: Government of Kenya
Has: Health Agents
HMN: Health Metrics Network
HSS: Health System Strengthening
HIS: Health Information System
IS: Information Systems
IT: Information Technology
KDHS: Kenya Demographic Health Survey
LMICs: Low and Middle Income Countries
MoH: Ministry of Health
MCUL: Master Community Units List
MIS: Management Information Systems
NGO: Non-Governmental Organization
SDGs: Sustainable Development Goals
SPSS: Statistical Package for Social Sciences
TAM: Technology Acceptance Model
WHO: World Health Organization
Acknowledgments
I acknowledge the contribution of each co-author, their support and availability for the process of achieving this study. All members of the community units Community Health Promoters and county leadership where this study drew the data are appreciated
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Aqil, A., Lippeveld, T., & Hozumi, D. (2009). PRISM framework: A paradigm shift for designing, strengthening and evaluating routine health information systems. Health Policy and Planning, 24(3), 217–228.
https://doi.org/10.1093/heapol/czp010
|
| [2] |
Cheburet, S., & Odhiambo-Otieno, G. (2016b). State of data quality of routing Health Management Information System: Case of Uasin Gishu County Referral Hospi tal, Kenya. International Research Journal of Public and Environmental Health, 3 (8), 174-181.
|
| [3] |
Chewicha, K. (2013). Community Health Information System for Family-centered Health Care: Scale-up in Southern Nations, Nationalities and People’s Region — MEASURE Evaluation. Retrieved August 30, 2017, from
https://www.measureevaluation.org/resources/publications/ja-13-161
|
| [4] |
Gilson, L., Daire, J., Patharath, A., & English, R. (2011). Leadership and governance within the South African health system. Durban: Health Systems Trust.
|
| [5] |
Haijden, J. G. (2009). Designing Management Information Systems. Oxford: Oxford University Press.
|
| [6] |
Jeremie N., Kaseje, D., Olayo, R., & Akinyi, C. (2014). Utilization of Community-based Health Information Systems in Decision Making and Health Action in Nyalenda, Kisumu County, Kenya. Universal Journal of Medical Science, 2(4), 37–42.
|
| [7] |
Kaburu, E., Kaburi, L., & Okero, D. (2016). Factors Influencing the Functionality of Community- Based Health Information Systems in Embakasi Sub- County, Nairobi County, Kenya. International Journal of Scientific and Research Publications, 6(5), 514-519.
|
| [8] |
Kibua, T. N., Muia, D. M., & Keraka, M. (2009). Efficacy of Community Based health care in Kenya: An evaluation of AMREF's 30 years in Kibwezi. AMREF Discussion Paper Series. Retrieved from
http://docplayer.net/54633214-Amref-discussion-paper-series-efficacy-of-community-based-health-care-in-kenya-an-evaluation-of-amref-s-30-years-in-kibwezi.html
|
| [9] |
Kihara, P. (2016). Strategy Implementation and Performance of Manufacturing Firms in Kenya. Latvia, European Union: Lap Lambert Academic Publishing.
|
| [10] |
Lehmann, U., & Matwa, P. (2008). Exploring the concept of power in the implementation of South Africa’s new community health worker policies: A case study from a rural sub-district. Discussion paper 64. Retrieved from
http://www.equinetafrica.org/sites/default/files/uploads/documents/DIS64POLlehmann.pdf
|
| [11] |
Mambo, S. N, Odhiambo-Otieno G. W, Ochieng’ Otieno G. and Wanja Mwaura T. (2021). Health systems strengthening: assessing the influence of organizational factors of community health volunteers on use of community based health information systems in selected counties, Kenya. International journal of community medicine and public health.
|
| [12] |
Mambo, S. N, Odhiambo-Otieno G. W, Ochieng’ Otieno G. and Wanja Mwaura T. (2018). Improving Health Systems: Influence of Technical Capacities of Community Health Volunteers on Use of Community Health Information Systems in Kenya. International Journal of Computer Applications (0975 – 8887) Volume 181 – No. 3, July 2018.
|
| [13] |
Mambo, S. N, Odhiambo-Otieno G. W, Ochieng’ Otieno G. and Wanja Mwaura T. (2018). Assessing the influence of process interventions of community health volunteers on use of Community Based Health Management Information Systems in selected Counties, Kenya.
http://www.ijsrp.org/research-journal-0818.php
|
| [14] |
Measure Evaluation (2009). Technical Consultation on Information Systems for Community-Based HIV Programs: MEASURE Evaluation. Retrieved August 30, 2017, from
https://www.measureevaluation.org/our-work/hiv-aids/community-based-hiv-info-systems/hiv-meeting-registration/folder_contents?show_all=true
|
| [15] |
Measure Evaluation. (2016). Community-based Health Information Systems in the Global Context: A Review of the Literature: MEASURE Evaluation. Retrieved March 26, 2018, from
https://www.measureevaluation.org/resources/publications/wp-16-161
|
| [16] |
Mbondenyi & Ambani (2014) The New Constitutional Law of Kenya. Principles, Government and Human Rights: Principles, Government and Human Rights.
|
| [17] |
Ministry of Health (2008). Collect, Manage, Visualize and Explore your Data. Retrieved November 4, 2016, from
https://www.dhis2.org/
|
| [18] |
Ministry of Health (2010). Microsoft Word - Community Strategy Evaluation report Retrieved November 4, 2016, from
http://www.unicef.org/evaldatabase/files/14_2010_HE_002_Community_Strategy_Evaluation_report_October_2010.pdf
|
| [19] |
Ministry of Health (2016). Kenya Master Health Facility List: Find all the health facilities in Kenya. Retrieved November 4, 2016, from
http://kmhfl.health.go.ke/#/home
|
| [20] |
Mugenda, O., & Mugenda, A. (2003). Research Methods: Quantitative and Qualitative Approaches. Nairobi: ACTS.
|
| [21] |
Naikal, A., & Chandra, S. (2013). Organisational Culture: A Case Study. Retrieved November 7, 2016, from
https://www.researchgate.net/publication/260094253_Organisational_Culture_A_Case_Study
|
| [22] |
Nutley, T. (2012). Improving Data Use in Decision Making: An Intervention to Strengthen Health Systems: MEASURE Evaluation. Retrieved November 4, 2016, from
https://www.measureevaluation.org/resources/publications/sr-12-73
|
| [23] |
Nzinga, J., Mbaabu, L., & English, M. (2013). Service delivery in Kenyan district hospitals–what can we learn from literature on mid-level managers? Human Resources for Health, 11(1), 1.
|
| [24] |
Odhiambo-Otieno, G. W., & Odero, W. W. (2005). Evaluation criteria for the district health management information systems: Lessons from the Ministry of Health, Kenya. African Health Sciences, 5(1), 59–64.
|
| [25] |
Pepela, W., & Odhiambo-Otieno, G. (2016). Community health information system utility: A case of Bungoma County Kenya. International Research Journal of Public and Environmental Health, 3(4), 75-86.
|
| [26] |
Vujicic, M., Ohiri, K., & Sparkes, S. (2009). Working in Health: Financing and Managing the Public Sector Health Workforce. Retrieved from
https://openknowledge.worldbank.org/handle/10986/2621
|
| [27] |
World Health Organization. (2007). Everybody’s business. Retrieved November 4, 2016, from
http://www.who.int/healthsystems/strategy/everybodys_business.pdf
|
| [28] |
World Health Organization. (2010). Monitoring the building blocks of health systems: A handbook of indicators and their measurement strategies. Retrieved November 4, 2016, from
http://www.who.int/healthinfo/systems/WHO_MBHSS_2010_full_web.pdf
|
Cite This Article
-
APA Style
Mambo, S. N., Odhiambo-Otieno, G., Ochieng’-Otieno, G., Mwaura-Tenambergen, W. (2024). Assessing the Influence of Behavioural Factors of Community Health Promoters on Use of Community Based Health Information Systems in Selected Counties, Kenya. World Journal of Public Health, 9(2), 95-110. https://doi.org/10.11648/j.wjph.20240902.11
 Copy
|
Copy
|
 Download
Download
ACS Style
Mambo, S. N.; Odhiambo-Otieno, G.; Ochieng’-Otieno, G.; Mwaura-Tenambergen, W. Assessing the Influence of Behavioural Factors of Community Health Promoters on Use of Community Based Health Information Systems in Selected Counties, Kenya. World J. Public Health 2024, 9(2), 95-110. doi: 10.11648/j.wjph.20240902.11
Copy
|
Download
AMA Style
Mambo SN, Odhiambo-Otieno G, Ochieng’-Otieno G, Mwaura-Tenambergen W. Assessing the Influence of Behavioural Factors of Community Health Promoters on Use of Community Based Health Information Systems in Selected Counties, Kenya. World J Public Health. 2024;9(2):95-110. doi: 10.11648/j.wjph.20240902.11
Copy
|
Download
-
@article{10.11648/j.wjph.20240902.11,
author = {Susan Njoki Mambo and George Odhiambo-Otieno and George Ochieng’-Otieno and Wanja Mwaura-Tenambergen},
title = {Assessing the Influence of Behavioural Factors of Community Health Promoters on Use of Community Based Health Information Systems in Selected Counties, Kenya
},
journal = {World Journal of Public Health},
volume = {9},
number = {2},
pages = {95-110},
doi = {10.11648/j.wjph.20240902.11},
url = {https://doi.org/10.11648/j.wjph.20240902.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.wjph.20240902.11},
abstract = {Globally, health management information systems (HMIS) in strengthening health systems have gained recognition due to potential of technology to improve access to quality care in underserved communities. In Kenya, the functionality of Community based- Health Management Information System (CBHMIS) currently stands at 55% down from 64% in year 2015. The aim of this paper was to determine the influence of behavioral factors of community units personnel on CBHMIS. As a nested study, with a broader aimt to establish the operational status of CBHMIS and its use in selected counties in Kenya; The main objective of this research was: To establish whether behavioural factors of Community Health Promoters (CHPs) influence CBHMIS use in Kenya. A mixed method design. was adopted, Kiambu, Kajiado and Nairobi counties formed the study location, a target population of 156 active community units was considered to arrive at a total sample of 122 community units and out of 7800CHPs a sample of 366 respondents was drawn. Multistage sampling was used to identify the CUs, and systematic random sampling to identify 366 respondents. Quantitative data tools were semi-structured closed ended questionnaires. Qualitative data tools included observation checklist, Focus Group Discussion and Key Informant Interviews guides. Quantitative data was analyzed using SPSS to generate univariate and bivariate analysis at p2 = .137). Results show that the model was valid (F(1, 363) = 58.579, P = .001) hence the explanatory variable (X2, Behavioral factors) is good in explaining total variations in Use of CbHMIS by community units. This implies that the use of CbHMIS by Community Units (CU) improves significantly when the community units have better behavioural factors. In conclusion, behavioural factors of CHPs have strong and significant influence on the CBHMIS use. Motivation of CHPs is key as a motivator to CBHMIS use, as well as. provision of material support including reporting tools and IEC materials and capacity development technical, computer and electronic reporting skills to enhamce CHP operations and processes.
},
year = {2024}
}
Copy
|
Download
-
TY - JOUR
T1 - Assessing the Influence of Behavioural Factors of Community Health Promoters on Use of Community Based Health Information Systems in Selected Counties, Kenya
AU - Susan Njoki Mambo
AU - George Odhiambo-Otieno
AU - George Ochieng’-Otieno
AU - Wanja Mwaura-Tenambergen
Y1 - 2024/04/28
PY - 2024
N1 - https://doi.org/10.11648/j.wjph.20240902.11
DO - 10.11648/j.wjph.20240902.11
T2 - World Journal of Public Health
JF - World Journal of Public Health
JO - World Journal of Public Health
SP - 95
EP - 110
PB - Science Publishing Group
SN - 2637-6059
UR - https://doi.org/10.11648/j.wjph.20240902.11
AB - Globally, health management information systems (HMIS) in strengthening health systems have gained recognition due to potential of technology to improve access to quality care in underserved communities. In Kenya, the functionality of Community based- Health Management Information System (CBHMIS) currently stands at 55% down from 64% in year 2015. The aim of this paper was to determine the influence of behavioral factors of community units personnel on CBHMIS. As a nested study, with a broader aimt to establish the operational status of CBHMIS and its use in selected counties in Kenya; The main objective of this research was: To establish whether behavioural factors of Community Health Promoters (CHPs) influence CBHMIS use in Kenya. A mixed method design. was adopted, Kiambu, Kajiado and Nairobi counties formed the study location, a target population of 156 active community units was considered to arrive at a total sample of 122 community units and out of 7800CHPs a sample of 366 respondents was drawn. Multistage sampling was used to identify the CUs, and systematic random sampling to identify 366 respondents. Quantitative data tools were semi-structured closed ended questionnaires. Qualitative data tools included observation checklist, Focus Group Discussion and Key Informant Interviews guides. Quantitative data was analyzed using SPSS to generate univariate and bivariate analysis at p2 = .137). Results show that the model was valid (F(1, 363) = 58.579, P = .001) hence the explanatory variable (X2, Behavioral factors) is good in explaining total variations in Use of CbHMIS by community units. This implies that the use of CbHMIS by Community Units (CU) improves significantly when the community units have better behavioural factors. In conclusion, behavioural factors of CHPs have strong and significant influence on the CBHMIS use. Motivation of CHPs is key as a motivator to CBHMIS use, as well as. provision of material support including reporting tools and IEC materials and capacity development technical, computer and electronic reporting skills to enhamce CHP operations and processes.
VL - 9
IS - 2
ER -
Copy
|
Download