Bouveret syndrome is one of the complications of gallstone disease possibly fatal, which is secondary to the presence of a large stone obliterating the lumen of the duodenum or stomach because of the formation of a cholecystoduodenal fistula. The gallstone reaches the duodenum through a bilioenteric fistula as a consequence of chronic inflammation and adherence between the gallbladder and the duodenum which increase the intraluminal pressure and leads to secondary wall ischemia and wall perforation with gallstone passage into the duodenum. Bouveret's syndrome's prevalence is highest among elderly women. Despite the rarity of Bouveret's syndrome, it can cause notable morbidity and mortality rates. We report a rare case of Bouveret's syndrome revealed by an unusual clinical picture of upper gastrointestinal bleeding in a 64-year-old patient. He had been admitted for significant gastrointestinal bleeding due to a probable antral stromal tumour. Endoscopic investigations had been inconclusive. An abdominal CT scan revealed a 72 x 43 mm mass in the second part of the duodenum in contact with the posterior wall of the stomach. Surgical exploration revealed a cholecystoduodenal fistula through which a large number of clots were passing, along with a huge stone measuring more than 7 cm inside the duodenum, extending up to the gastric antrum. After antroduodenotomy, we discovered almost complete erosion of D1 by the stone, which explained the haemorrhages. An antroduodenectomy (D1) was performed due to the parietal destruction of D1 and the very high risk of haemorrhage. The outcome was favourable. The medical history revealed a history of a large untreated gallstone.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Bouveret syndrome is a very rare form of gastric obstruction secondary to the passage of a gallstone into the duodenum through a cholecystoduodenal fistula
[1]
Jobin Philipose, Hafiz M Khan, Moiz Ahmed, Pretty S Idiculla, Sherif Andrawes, Bouveret's Syndrome. Cureus 2019 Apr 9; 11(4): e4414.
. It is a rare complication of gallstone disease that usually presents with signs and symptoms of gastric outlet obstruction
[2]
Kelly M Caldwell, Seeyuen J Lee, Phillip L Leggett, Kulvinder S Bajwa, Sheilendra S Mehta, Shinil K Shah. Bouveret syndrome: current management strategies. Clin Exp Gastroenterol. 2018 Feb 15; 11: 69–75.
. We report a rare case of Bouveret's syndrome revealed by an unusual presentation of upper gastrointestinal bleeding in a 64-year-old man.
2. Case Report
A 64-year-old man was referred to the visceral surgery department for significant gastrointestinal bleeding due to a probable antral stromal tumour. Patient is on antihypertensivee medications.
Two weeks earlier, he had been admitted to the gastroenterology department for the first time for repeated episodes of low-volume haematemesis associated with melena and epigastric pain, which had been ongoing for two months.
During this initial hospitalisation, investigations revealed anaemia at 8.10 g/dl and, on oesophagogastroduodenal fibroscopy, an ulcer on the posterior surface of the Forrest III bulb and at the top of D1 stage IIb, which were treated medically with favourable results and discharged with an appointment for follow-up.
One week after his discharge, he experienced a recurrence of hematemesis, which became very profuse, with significant asthenia and patient dyspepsia. This led to a second hospitalisation in the gastroenterology department.
Due to persistent gastrointestinal bleeding and severe anaemia at 6 g/dl despite repeated transfusions, he was admitted to the operating theatre on an emergency basis by the surgeon on call for surgical haemostasis.
During the operation, this initial attempt at haemostasis was blocked by a massive, telescoped appearance of the antro-duodenal region with the liver, hepatic pedicle and head of the pancreas, which was considered to be a stromal tumour affecting the head of the pancreas. An attempt at resection would have been perilous in emergency conditions.
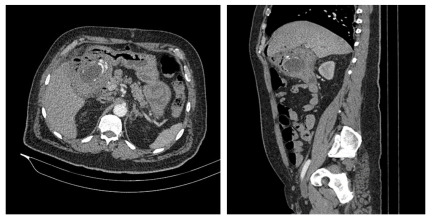
Further investigation was then carried out using abdominal computed tomography, which showed a hypodense mass located in the second duodenal portion D2 measuring 72 x 43 mm in contact with the posterior wall of the stomach, which it was pushing back with infiltration of the perilesional fat (Figure 1).
Figure 1. Abdominal scan showing a mass in the duodenal region.
In this context, he was referred to us for gastrointestinal bleeding due to probable GIST and was prepared for major surgery.
We had scheduled the patient for possible extended resection, which might require cephalic duodenopancreatectomy.
The approach was a repeat median laparotomy.
During exploration, we found a large mass occupying the entire duodenum, greater omentum and right colic angle, all pressed against the head of the pancreas and liver.
The gallbladder was not visible at first glance. After separating it from the liver, we realised that it was sclerotic and atrophic.
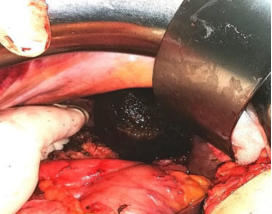
Subsequently, a cholecystoduodenal fistula was identified, through which a large number of clots were passing, and a huge stone was discovered inside the duodenum, extending up to the gastric antrum, which was responsible for this mass effect.
An antroduodenotomy was performed, revealing almost complete erosion of D1 by the stone, which explained the haemorrhages (Figures 2 and 3).
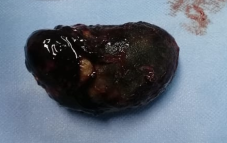
After extracting the stone, we noticed that the posterior wall of D1, particularly the bulb, was completely destroyed, exposing the gastroduodenal artery. Having ruled out a tumour as the cause, the only sure way to eliminate the risk of haemorrhage was to perform a resection with ligation of the gastroduodenal artery. This resection first required the removal of D1 up to the superior flexure. Next, a gastro-duodenectomy with monobloc cholecystectomy was performed (Figure 4), allowing resection of the area of duodenal wall destruction. Finally, a terminolateral gastro-jejunal anastomosis was performed.
The medical history subsequently revealed the presence of a large gallstone that had not been treated. The patient remained in the intensive care unit for 48 hours for post-operative monitoring. The post-operative course was uneventful, with bowel function returning on day 3, refeeding on day 6 with good tolerance, and discharge on day 7 post-operatively.
3. Discusssion
In this case report, we present a case of Bouveret’s syndrome complicated by upper gastrointestinal haemorrhage.
This rare syndrome describes obstruction of a gallstone in the pylorus or dodenum secondary to a cholecysto-duodenal fistula
[3]
Bhandari, Tika Ram, John Lin Hieng Wong et al. Bouveret’s Syndrome: An Old Diagnosis. A Modern Multimodality Approach (Endoscopic And Robotic Surgical) Of Gastric Outlet Obstruction: Report Of Two Cases. International Journal Of Surgery Case Reports. 2024, 114(December 2023), 109134. Available Z:
Kabir, Kaiser F, John P Hanna A Hossein Haghbin. No Stone Left Unturned: Bouveret Syndrome Treated With Electrohydraulic Lithotripsy And Open Extraction With Pyloric Exclusion And Gastrojejunostomy. Cureus. 2023, 15(5). Available Z:
. Historically, it was first reported in 1770 by the French physician Beaussier, and in 1896 it was named after the French physician Leon August Bouveret, who reported two cases in the Revue de Médecine
[3]
Bhandari, Tika Ram, John Lin Hieng Wong et al. Bouveret’s Syndrome: An Old Diagnosis. A Modern Multimodality Approach (Endoscopic And Robotic Surgical) Of Gastric Outlet Obstruction: Report Of Two Cases. International Journal Of Surgery Case Reports. 2024, 114(December 2023), 109134. Available Z:
Physiopathologically, the formation of the fistula is a consequence of chronic inflammation with adhesion of the gallbladder to the gastrointestinal tract and parietal ischaemia secondary to the mechanical pressure exerted by the stones on the vesicular and intestinal walls. This ischaemia is followed by the formation of a fistula between the gallbladder and the intestine
[4]
Haddad, Fady G., Wissam Mansour A Liliane Deeb et al. Bouveret’s Syndrome: Literature Review. Cureus. 2018, 10(3), 3–6. Dostupné Z:
Anisha R.; Pujitha Kudaravalli; JasimH. Al-Musawi; Hira Ahmad. Bouveret Syndrome bilioduodenal fistula). National Library Of Medicine, (online). March 13, 2023.
[8]
Hakima Abib, Fatima Babakhouya, Ahmed Zerhouni et al. Ileus biliaris: a rare cause of intestinal obstruction, case report. Pan African Medical Journal.
Karim Osman, Daniel Maselli, Ayse Tuba Kendi, Mark Larson. Bouveret’s syndrome and cholecystogastric fistula: a case‑report and review of the literature. Clinical Journal of Gastroenterology. Japanese Society of Gastroenterology 2020.
. Gallstones can then migrate to different parts of the digestive tract, namely the ileocecal region (50%–90%), the jejunum and ileum (20%–40%), and more rarely the stomach or duodenum (<5%), in which case it is referred to as Bouveret's syndrome
[10]
Philipp Kasper, Daniele Palmisano, Uwe Janssens et al. Acute gastric outlet obstruction due to an impacted gallstone: the Bouveret’s syndrome. BMJ Case Report 2021; 14: e242301.
Our patient, who was 64 years old with a history of gallstones that was discovered retrospectively during the medical history interview and a stone measuring more than 7 cm in diameter that was extracted, had three of the four risk factors for Bouveret's syndrome described in the literature (age > 60 years, history of gallstones, large stone measuring 7 cm). The final risk factor is female gender
[5]
Anisha R.; Pujitha Kudaravalli; JasimH. Al-Musawi; Hira Ahmad. Bouveret Syndrome bilioduodenal fistula). National Library Of Medicine, (online). March 13, 2023.
[5]
.
The initial clinical presentation in our case was upper gastrointestinal bleeding. This is a rare and unusual clinical presentation
[11]
Brice R, et al. A rare cause of hematemesis. Rev Med Internal (2014),
Alaa Abou-Saif et al. Complications of Gallstone Disease: Mirizzi Syndrome, Cholecystocholedochal Fistula and Gallstone Ileus. The American Journal of Gastroenterology.
[16]
Elmer Hoekstra, Maarte, Willem van den Berg, Roeland Andreas Veenendaal, Rogier Stuyt. The natural progression of a fistulizing gallstone resulting in massive gastrointestinal hemmorhage and Bouveret syndrome, a rare case. Clinical Journal o Gastroenterology, (2020) 13: 393-396.
. However, this remains an exceptional mode of discovery, because Bouveret's syndrome most often presents with a triad of epigastric pain, nausea and vomiting. It can also present with abdominal pain, distension, fever, weight loss and anorexia
[11]
Brice R, et al. A rare cause of hematemesis. Rev Med Internal (2014),
Karim Osman, Daniel Maselli, Ayse Tuba Kendi, Mark Larson. Bouveret’s syndrome and cholecystogastric fistula: a case‑report and review of the literature. Clinical Journal of Gastroenterology. Japanese Society of Gastroenterology 2020.
. The latter two symptoms were also found in the case we presented, along with significant asthenia and patient dyspepsia. In addition to upper gastrointestinal haemorrhage, the second mode of presentation in the case described above is pseudotumoral.
These two presentation patterns can cause diagnostic difficulties. In our patient, endoscopic examinations performed in response to upper gastrointestinal bleeding were inconclusive; and the persistence of significant bleeding necessitated an initial emergency surgery, during which a pseudomass was discovered in the antroduodenal region, covering the inferior surface of the liver, the hepatic pedicle and the head of the pancreas. This was considered to be a gastrointestinal stromal tumour, which could not be resected in an emergency setting. Subsequent imaging, particularly abdominal computed tomography, did not reveal Rigler's triad, which is suggestive of Bouveret's syndrome, namely aerobilia, ectopic calculus and high-level obstruction
[4]
Haddad, Fady G., Wissam Mansour A Liliane Deeb et al. Bouveret’s Syndrome: Literature Review. Cureus. 2018, 10(3), 3–6. Dostupné Z:
. Instead, it suggested a hypodense mass in the second duodenum. Moreover, a comprehensive review of cases in the literature recently published that only 24% of patients have a choledochoduodenal fistula visible on CT scan, and gallstones are visible during oesophagogastroduodenoscopy in approximately 69% of reported cases
[7]
Kabir, Kaiser F, John P Hanna A Hossein Haghbin. No Stone Left Unturned: Bouveret Syndrome Treated With Electrohydraulic Lithotripsy And Open Extraction With Pyloric Exclusion And Gastrojejunostomy. Cureus. 2023, 15(5). Available Z:
The diagnosis of Bouveret's syndrome is based on clinical presentation and imaging. In many cases, this diagnosis is difficult to make using imaging, and endoscopy offers no advantage. Surgery is therefore the diagnostic and therapeutic modality of choice
[4]
Haddad, Fady G., Wissam Mansour A Liliane Deeb et al. Bouveret’s Syndrome: Literature Review. Cureus. 2018, 10(3), 3–6. Dostupné Z:
. Indeed, in our patient, the diagnosis could only be made intraoperatively despite the imaging and endoscopy examinations performed prior to the procedure.
In terms of treatment, the patient underwent preoperative preparation as he had been scheduled for a possible extended resection of the mass, which could require a cephalic duodenopancreatectomy. During the operation, a cholecystoduodenal fistula was discovered, through which a large number of clots were passing, revealing a huge stone inside the duodenum extending up to the gastric antrum, with almost complete destruction of D1 by the stone, explaining the haemorrhages. We extracted the large stone and performed a gastroduodenectomy to resect the irreversibly damaged parts of the duodenum and stomach (Figure 3) and to achieve haemostasis. Indeed, other authors, such as Brice et al., have also mentioned the need for resection in cases of irreversibly damaged structures. Bouveret's syndrome is usually treated surgically with removal of the obstructive stone
[11]
Brice R, et al. A rare cause of hematemesis. Rev Med Internal (2014),
. The surgical approach consists of a gastrotomy, an antropylorotomy or a duodenotomy. In the case of a distal stone or a stone that has migrated to the proximal part of the jejunum, an enterotomy centred on the stone will allow the stone to be removed. The distal part of the small intestine must be examined to ensure that no other large migrated stones could cause postoperative ileus. The morbidity and mortality rates of open surgery reported by some authors are 37.5% and 11% respectively. Apart from open surgery, there is minimally invasive treatment, which includes endoscopic retrieval, mechanical lithotripsy, electrohydraulic lithotripsy, laser lithotripsy and extracorporeal shock wave lithotripsy
[5]
Anisha R.; Pujitha Kudaravalli; JasimH. Al-Musawi; Hira Ahmad. Bouveret Syndrome bilioduodenal fistula). National Library Of Medicine, (online). March 13, 2023.
[5]
. Endoscopic stone removal with or without fragmentation by mechanical or extracorporeal lithotripsy is a therapeutic alternative for stones smaller than 2.5 cm and not impacted
[11]
Brice R, et al. A rare cause of hematemesis. Rev Med Internal (2014),
Various reports of successful endoscopic removal have also been published in the literature. However, these only concern stones that are generally smaller than 4 cm
[15]
Hendriks, Sofie, Mareille Maria Verseveld et al. Successful Endoscopic Treatment Of A Large Impacted Gallstone In The Duodenum Using Laser Lithotripsy, Bouveret’s Syndrome: A Case Report. World Journal Of Gastroenterology. 2020, 26(19), 2458–2463. Available Z:
The progression of Bouveret's syndrome depends mainly on the timing of diagnosis and the speed of treatment. In our case, it was satisfactory. The prognosis is generally good
[5]
Anisha R.; Pujitha Kudaravalli; JasimH. Al-Musawi; Hira Ahmad. Bouveret Syndrome bilioduodenal fistula). National Library Of Medicine, (online). March 13, 2023.
[5]
, however, some authors have reported mortality rates in this syndrome of up to 33%
[10]
Philipp Kasper, Daniele Palmisano, Uwe Janssens et al. Acute gastric outlet obstruction due to an impacted gallstone: the Bouveret’s syndrome. BMJ Case Report 2021; 14: e242301.
Dong, Matthew, Alfredo Daniel Guerron et al. Choleduodenal Fistula With Gastric Outlet Obstruction. Bmj Case Reports. 2016, 2016, 2015–2017. Available Z:
We treated a rare complication of gallstone disease. The presentation of Bouveret's syndrome with upper gastrointestinal haemorrhage in a life-threatening emergency initially suggested a GIST based on the CT scan. Surgical exploration allowed the diagnosis to be corrected and an antroduodenectomy (D1) to be performed due to the parietal destruction of D1 and the very high risk of haemorrhage. The outcome was favourable.
Kelly M Caldwell, Seeyuen J Lee, Phillip L Leggett, Kulvinder S Bajwa, Sheilendra S Mehta, Shinil K Shah. Bouveret syndrome: current management strategies. Clin Exp Gastroenterol. 2018 Feb 15; 11: 69–75.
Bhandari, Tika Ram, John Lin Hieng Wong et al. Bouveret’s Syndrome: An Old Diagnosis. A Modern Multimodality Approach (Endoscopic And Robotic Surgical) Of Gastric Outlet Obstruction: Report Of Two Cases. International Journal Of Surgery Case Reports. 2024, 114(December 2023), 109134. Available Z:
Kabir, Kaiser F, John P Hanna A Hossein Haghbin. No Stone Left Unturned: Bouveret Syndrome Treated With Electrohydraulic Lithotripsy And Open Extraction With Pyloric Exclusion And Gastrojejunostomy. Cureus. 2023, 15(5). Available Z:
Hakima Abib, Fatima Babakhouya, Ahmed Zerhouni et al. Ileus biliaris: a rare cause of intestinal obstruction, case report. Pan African Medical Journal.
Karim Osman, Daniel Maselli, Ayse Tuba Kendi, Mark Larson. Bouveret’s syndrome and cholecystogastric fistula: a case‑report and review of the literature. Clinical Journal of Gastroenterology. Japanese Society of Gastroenterology 2020.
Philipp Kasper, Daniele Palmisano, Uwe Janssens et al. Acute gastric outlet obstruction due to an impacted gallstone: the Bouveret’s syndrome. BMJ Case Report 2021; 14: e242301.
Alaa Abou-Saif et al. Complications of Gallstone Disease: Mirizzi Syndrome, Cholecystocholedochal Fistula and Gallstone Ileus. The American Journal of Gastroenterology.
[14]
Dong, Matthew, Alfredo Daniel Guerron et al. Choleduodenal Fistula With Gastric Outlet Obstruction. Bmj Case Reports. 2016, 2016, 2015–2017. Available Z:
Hendriks, Sofie, Mareille Maria Verseveld et al. Successful Endoscopic Treatment Of A Large Impacted Gallstone In The Duodenum Using Laser Lithotripsy, Bouveret’s Syndrome: A Case Report. World Journal Of Gastroenterology. 2020, 26(19), 2458–2463. Available Z:
Elmer Hoekstra, Maarte, Willem van den Berg, Roeland Andreas Veenendaal, Rogier Stuyt. The natural progression of a fistulizing gallstone resulting in massive gastrointestinal hemmorhage and Bouveret syndrome, a rare case. Clinical Journal o Gastroenterology, (2020) 13: 393-396.
Bidzo, M. C. N., Faraj, M. R., Boulghmair, A., Kissi, K., Kwedi, A. M. N., et al. (2026). Upper Gastrointestinal Bleeding of Rare Cause: A Case Report and Literature Review. World Journal of Medical Case Reports, 7(1), 18-22. https://doi.org/10.11648/j.wjmcr.20260701.15
Bidzo, M. C. N.; Faraj, M. R.; Boulghmair, A.; Kissi, K.; Kwedi, A. M. N., et al. Upper Gastrointestinal Bleeding of Rare Cause: A Case Report and Literature Review. World J. Med. Case Rep.2026, 7(1), 18-22. doi: 10.11648/j.wjmcr.20260701.15
Bidzo MCN, Faraj MR, Boulghmair A, Kissi K, Kwedi AMN, et al. Upper Gastrointestinal Bleeding of Rare Cause: A Case Report and Literature Review. World J Med Case Rep. 2026;7(1):18-22. doi: 10.11648/j.wjmcr.20260701.15
@article{10.11648/j.wjmcr.20260701.15,
author = {Mariette Cecile Nsa Bidzo and Mohammed Rachid Faraj and Anass Boulghmair and Kenza Kissi and Alexandra Maeva Nguinya Kwedi and Saad Al Baroudi},
title = {Upper Gastrointestinal Bleeding of Rare Cause: A Case Report and Literature Review},
journal = {World Journal of Medical Case Reports},
volume = {7},
number = {1},
pages = {18-22},
doi = {10.11648/j.wjmcr.20260701.15},
url = {https://doi.org/10.11648/j.wjmcr.20260701.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.wjmcr.20260701.15},
abstract = {Bouveret syndrome is one of the complications of gallstone disease possibly fatal, which is secondary to the presence of a large stone obliterating the lumen of the duodenum or stomach because of the formation of a cholecystoduodenal fistula. The gallstone reaches the duodenum through a bilioenteric fistula as a consequence of chronic inflammation and adherence between the gallbladder and the duodenum which increase the intraluminal pressure and leads to secondary wall ischemia and wall perforation with gallstone passage into the duodenum. Bouveret's syndrome's prevalence is highest among elderly women. Despite the rarity of Bouveret's syndrome, it can cause notable morbidity and mortality rates. We report a rare case of Bouveret's syndrome revealed by an unusual clinical picture of upper gastrointestinal bleeding in a 64-year-old patient. He had been admitted for significant gastrointestinal bleeding due to a probable antral stromal tumour. Endoscopic investigations had been inconclusive. An abdominal CT scan revealed a 72 x 43 mm mass in the second part of the duodenum in contact with the posterior wall of the stomach. Surgical exploration revealed a cholecystoduodenal fistula through which a large number of clots were passing, along with a huge stone measuring more than 7 cm inside the duodenum, extending up to the gastric antrum. After antroduodenotomy, we discovered almost complete erosion of D1 by the stone, which explained the haemorrhages. An antroduodenectomy (D1) was performed due to the parietal destruction of D1 and the very high risk of haemorrhage. The outcome was favourable. The medical history revealed a history of a large untreated gallstone.},
year = {2026}
}
TY - JOUR
T1 - Upper Gastrointestinal Bleeding of Rare Cause: A Case Report and Literature Review
AU - Mariette Cecile Nsa Bidzo
AU - Mohammed Rachid Faraj
AU - Anass Boulghmair
AU - Kenza Kissi
AU - Alexandra Maeva Nguinya Kwedi
AU - Saad Al Baroudi
Y1 - 2026/03/19
PY - 2026
N1 - https://doi.org/10.11648/j.wjmcr.20260701.15
DO - 10.11648/j.wjmcr.20260701.15
T2 - World Journal of Medical Case Reports
JF - World Journal of Medical Case Reports
JO - World Journal of Medical Case Reports
SP - 18
EP - 22
PB - Science Publishing Group
SN - 2994-726X
UR - https://doi.org/10.11648/j.wjmcr.20260701.15
AB - Bouveret syndrome is one of the complications of gallstone disease possibly fatal, which is secondary to the presence of a large stone obliterating the lumen of the duodenum or stomach because of the formation of a cholecystoduodenal fistula. The gallstone reaches the duodenum through a bilioenteric fistula as a consequence of chronic inflammation and adherence between the gallbladder and the duodenum which increase the intraluminal pressure and leads to secondary wall ischemia and wall perforation with gallstone passage into the duodenum. Bouveret's syndrome's prevalence is highest among elderly women. Despite the rarity of Bouveret's syndrome, it can cause notable morbidity and mortality rates. We report a rare case of Bouveret's syndrome revealed by an unusual clinical picture of upper gastrointestinal bleeding in a 64-year-old patient. He had been admitted for significant gastrointestinal bleeding due to a probable antral stromal tumour. Endoscopic investigations had been inconclusive. An abdominal CT scan revealed a 72 x 43 mm mass in the second part of the duodenum in contact with the posterior wall of the stomach. Surgical exploration revealed a cholecystoduodenal fistula through which a large number of clots were passing, along with a huge stone measuring more than 7 cm inside the duodenum, extending up to the gastric antrum. After antroduodenotomy, we discovered almost complete erosion of D1 by the stone, which explained the haemorrhages. An antroduodenectomy (D1) was performed due to the parietal destruction of D1 and the very high risk of haemorrhage. The outcome was favourable. The medical history revealed a history of a large untreated gallstone.
VL - 7
IS - 1
ER -
Bidzo, M. C. N., Faraj, M. R., Boulghmair, A., Kissi, K., Kwedi, A. M. N., et al. (2026). Upper Gastrointestinal Bleeding of Rare Cause: A Case Report and Literature Review. World Journal of Medical Case Reports, 7(1), 18-22. https://doi.org/10.11648/j.wjmcr.20260701.15
Bidzo, M. C. N.; Faraj, M. R.; Boulghmair, A.; Kissi, K.; Kwedi, A. M. N., et al. Upper Gastrointestinal Bleeding of Rare Cause: A Case Report and Literature Review. World J. Med. Case Rep.2026, 7(1), 18-22. doi: 10.11648/j.wjmcr.20260701.15
Bidzo MCN, Faraj MR, Boulghmair A, Kissi K, Kwedi AMN, et al. Upper Gastrointestinal Bleeding of Rare Cause: A Case Report and Literature Review. World J Med Case Rep. 2026;7(1):18-22. doi: 10.11648/j.wjmcr.20260701.15
@article{10.11648/j.wjmcr.20260701.15,
author = {Mariette Cecile Nsa Bidzo and Mohammed Rachid Faraj and Anass Boulghmair and Kenza Kissi and Alexandra Maeva Nguinya Kwedi and Saad Al Baroudi},
title = {Upper Gastrointestinal Bleeding of Rare Cause: A Case Report and Literature Review},
journal = {World Journal of Medical Case Reports},
volume = {7},
number = {1},
pages = {18-22},
doi = {10.11648/j.wjmcr.20260701.15},
url = {https://doi.org/10.11648/j.wjmcr.20260701.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.wjmcr.20260701.15},
abstract = {Bouveret syndrome is one of the complications of gallstone disease possibly fatal, which is secondary to the presence of a large stone obliterating the lumen of the duodenum or stomach because of the formation of a cholecystoduodenal fistula. The gallstone reaches the duodenum through a bilioenteric fistula as a consequence of chronic inflammation and adherence between the gallbladder and the duodenum which increase the intraluminal pressure and leads to secondary wall ischemia and wall perforation with gallstone passage into the duodenum. Bouveret's syndrome's prevalence is highest among elderly women. Despite the rarity of Bouveret's syndrome, it can cause notable morbidity and mortality rates. We report a rare case of Bouveret's syndrome revealed by an unusual clinical picture of upper gastrointestinal bleeding in a 64-year-old patient. He had been admitted for significant gastrointestinal bleeding due to a probable antral stromal tumour. Endoscopic investigations had been inconclusive. An abdominal CT scan revealed a 72 x 43 mm mass in the second part of the duodenum in contact with the posterior wall of the stomach. Surgical exploration revealed a cholecystoduodenal fistula through which a large number of clots were passing, along with a huge stone measuring more than 7 cm inside the duodenum, extending up to the gastric antrum. After antroduodenotomy, we discovered almost complete erosion of D1 by the stone, which explained the haemorrhages. An antroduodenectomy (D1) was performed due to the parietal destruction of D1 and the very high risk of haemorrhage. The outcome was favourable. The medical history revealed a history of a large untreated gallstone.},
year = {2026}
}
TY - JOUR
T1 - Upper Gastrointestinal Bleeding of Rare Cause: A Case Report and Literature Review
AU - Mariette Cecile Nsa Bidzo
AU - Mohammed Rachid Faraj
AU - Anass Boulghmair
AU - Kenza Kissi
AU - Alexandra Maeva Nguinya Kwedi
AU - Saad Al Baroudi
Y1 - 2026/03/19
PY - 2026
N1 - https://doi.org/10.11648/j.wjmcr.20260701.15
DO - 10.11648/j.wjmcr.20260701.15
T2 - World Journal of Medical Case Reports
JF - World Journal of Medical Case Reports
JO - World Journal of Medical Case Reports
SP - 18
EP - 22
PB - Science Publishing Group
SN - 2994-726X
UR - https://doi.org/10.11648/j.wjmcr.20260701.15
AB - Bouveret syndrome is one of the complications of gallstone disease possibly fatal, which is secondary to the presence of a large stone obliterating the lumen of the duodenum or stomach because of the formation of a cholecystoduodenal fistula. The gallstone reaches the duodenum through a bilioenteric fistula as a consequence of chronic inflammation and adherence between the gallbladder and the duodenum which increase the intraluminal pressure and leads to secondary wall ischemia and wall perforation with gallstone passage into the duodenum. Bouveret's syndrome's prevalence is highest among elderly women. Despite the rarity of Bouveret's syndrome, it can cause notable morbidity and mortality rates. We report a rare case of Bouveret's syndrome revealed by an unusual clinical picture of upper gastrointestinal bleeding in a 64-year-old patient. He had been admitted for significant gastrointestinal bleeding due to a probable antral stromal tumour. Endoscopic investigations had been inconclusive. An abdominal CT scan revealed a 72 x 43 mm mass in the second part of the duodenum in contact with the posterior wall of the stomach. Surgical exploration revealed a cholecystoduodenal fistula through which a large number of clots were passing, along with a huge stone measuring more than 7 cm inside the duodenum, extending up to the gastric antrum. After antroduodenotomy, we discovered almost complete erosion of D1 by the stone, which explained the haemorrhages. An antroduodenectomy (D1) was performed due to the parietal destruction of D1 and the very high risk of haemorrhage. The outcome was favourable. The medical history revealed a history of a large untreated gallstone.
VL - 7
IS - 1
ER -