A 62-year-old Iraqi woman exhibited progressive enlargement of her hands, feet, and facial features over several years, accompanied by poorly controlled type 2 diabetes mellitus, hypertension, and dyslipidemia—metabolic disorders that had become increasingly challenging to manage despite conventional treatment. These gradual physical changes, which are often very small in middle-aged and older people, eventually made doctors think that the person might have acromegaly. Biochemical testing confirmed the diagnosis by showing consistently high levels of growth hormone, no suppression on oral glucose tolerance testing, and insulin-like growth factor-1 concentrations that were much higher than normal for someone of the same age and sex. A macroadenoma measuring 14 × 12 × 9 mm was found on a pituitary magnetic resonance imaging scan. There was no suprasellar extension, optic chiasm compression, or visual field problems on formal testing. After a thorough discussion of treatment options, the patient opted against transsphenoidal surgery, citing personal preference and apprehensions about surgical risks, and instead chose to initiate primary medical treatment. She began taking Sandostatin LAR (octreotide), a long-acting somatostatin receptor ligand, at a low dose that was gradually increased over the next few months based on how well she tolerated it and how her biochemical response changed. Regular follow-up lab tests showed that insulin-like growth factor-1 levels were steadily dropping toward the normal range. This showed that the excess growth hormone was being successfully suppressed. A follow-up MRI about a year into treatment showed a good response, with the adenoma getting smaller and cystic degeneration appearing in the tumor, which is what you would expect from somatostatin analog–mediated regression. This hormonal enhancement was accompanied by improved management of her metabolic comorbidities, including enhanced glycemic control, lowered blood pressure, and optimized lipid profiles, highlighting the close association between acromegaly and cardiometabolic complications. This case underscores the necessity of early recognition of acromegaly in patients primarily exhibiting metabolic disturbances and subtle physical manifestations, particularly when surgical intervention is not feasible. It also shows how effective somatostatin analogs can be as a powerful nonsurgical treatment that can help with biochemical control, tumor reduction, and overall metabolic health. In these cases, successful management depends on a personalized, multidisciplinary framework that includes regular endocrinological evaluations, hormonal monitoring, and periodic imaging. This is done to get the best disease control, reduce long-term complications, and improve quality of life.
| Published in | Science Discovery Medicine (Volume 1, Issue 1) |
| DOI | 10.11648/j.sdmed.20260101.14 |
| Page(s) | 19-23 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Acromegaly, Pituitary Macroadenoma, Octreotide, Somatostatin Analog, IGF-1, Medical Management
GH | Growth Hormone |
IGF-1 | Insulin-Like Growth Factor-1 |
MRI | Magnetic Resonance Imaging |
SRLs | Somatostatin Receptor Ligands |
IM | Intramuscular |
DM | Diabetes Mellitus |
T1WI | T1-Weighted Imaging |
T2WI | T2-Weighted Imaging |
FLAIR | Fluid-Attenuated Inversion Recovery |
DWI | Diffusion-Weighted Imaging |
ADC | Apparent Diffusion Coefficient |
SRL | Somatostatin Receptor Ligand |
GHRA | Growth Hormone Receptor Antagonist |
| [1] | Melmed S. Acromegaly. N Engl J Med. 2020; 382(10): 944–956. |
| [2] | Gadelha MR, Kasuki L, Lim DST, Fleseriu M. Systemic complications of acromegaly and the impact of the current treatment landscape: an update. Endocr Rev. 2019; 40(1): 268–332. |
| [3] | Holdaway IM, Bolland MJ, Gamble GD. A meta-analysis of the effect of lowering serum levels of GH and IGF-1 on mortality in acromegaly. Eur J Endocrinol. 2008; 159(2): 89–95. |
| [4] | Giustina A, Barkhoudarian G, Beckers A, et al. Multidisciplinary management of acromegaly: a consensus. Rev Endocr Metab Disord. 2020; 21(4): 667–678. |
| [5] | Fleseriu M, Hashim IA, Karavitaki N, Melmed S, Murad MH, Salvatori R, et al. Hormonal replacement in hypopituitarism in adults: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2016; 101(11): 3888–3921. |
| [6] | Katznelson L, Laws ER Jr, Melmed S, Molitch ME, Murad MH, Utz A, et al. Acromegaly: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2014; 99(11): 3933–3951. |
| [7] | Melmed S. Medical progress: Acromegaly. N Engl J Med. 2006; 355(24): 2558–2573. |
| [8] | Ershadinia N, Tritos NA. Diagnosis and treatment of acromegaly: an update. Mayo Clin Proc. 2022; 97(2): 333–346. |
| [9] | Fleseriu M, Langlois F, Lim DST, Varlamov EV, Melmed S. Acromegaly: pathogenesis, diagnosis, and management. Lancet Diabetes Endocrinol. 2022; 10(11): 804–826. |
| [10] | Puig-Domingo M, Bernabéu I, Picó A, et al. Pasireotide in the personalized treatment of acromegaly. Front Endocrinol (Lausanne). 2021; 12: 648411. |
| [11] | Samson SL. Is diabetes with acromegaly for life? Pituitary. 2024; 27(5): 433–436. |
| [12] | Biermasz N, Fleseriu M, Dreval AV, et al. Oral octreotide capsules lowered incidence and improved severity of acromegaly symptoms compared with injectable somatostatin receptor ligands: results from the MPOWERED trial. Endocrine Abstracts. 2021; 73: PEP8. 1. |
| [13] | Giustina A, Biermasz N, Casanueva FF, et al. Consensus on criteria for acromegaly diagnosis and remission. Pituitary. 2024; 27(1): 7–22. |
| [14] | McGovern G. FDA accepts NDA for paltusotine to treat adult patients with acromegaly. Pharmacy Times. Published December 9, 2024. |
APA Style
Shehata, A., Aijaz, A., Ibrar, I., Gouher, A., Shahbaz, M. K., et al. (2026). Medical Management of Acromegaly in a Middle-aged Woman with Pituitary Macroadenoma and Metabolic Comorbidities: A Case Report. Science Discovery Medicine, 1(1), 19-23. https://doi.org/10.11648/j.sdmed.20260101.14
ACS Style
Shehata, A.; Aijaz, A.; Ibrar, I.; Gouher, A.; Shahbaz, M. K., et al. Medical Management of Acromegaly in a Middle-aged Woman with Pituitary Macroadenoma and Metabolic Comorbidities: A Case Report. Sci. Discov. Med. 2026, 1(1), 19-23. doi: 10.11648/j.sdmed.20260101.14
@article{10.11648/j.sdmed.20260101.14,
author = {Abdelrahman Shehata and Ayesha Aijaz and Ibrahim Ibrar and Abia Gouher and Muhammad Kamil Shahbaz and Mahir Jallo},
title = {Medical Management of Acromegaly in a Middle-aged Woman with Pituitary Macroadenoma and Metabolic Comorbidities: A Case Report},
journal = {Science Discovery Medicine},
volume = {1},
number = {1},
pages = {19-23},
doi = {10.11648/j.sdmed.20260101.14},
url = {https://doi.org/10.11648/j.sdmed.20260101.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.sdmed.20260101.14},
abstract = {A 62-year-old Iraqi woman exhibited progressive enlargement of her hands, feet, and facial features over several years, accompanied by poorly controlled type 2 diabetes mellitus, hypertension, and dyslipidemia—metabolic disorders that had become increasingly challenging to manage despite conventional treatment. These gradual physical changes, which are often very small in middle-aged and older people, eventually made doctors think that the person might have acromegaly. Biochemical testing confirmed the diagnosis by showing consistently high levels of growth hormone, no suppression on oral glucose tolerance testing, and insulin-like growth factor-1 concentrations that were much higher than normal for someone of the same age and sex. A macroadenoma measuring 14 × 12 × 9 mm was found on a pituitary magnetic resonance imaging scan. There was no suprasellar extension, optic chiasm compression, or visual field problems on formal testing. After a thorough discussion of treatment options, the patient opted against transsphenoidal surgery, citing personal preference and apprehensions about surgical risks, and instead chose to initiate primary medical treatment. She began taking Sandostatin LAR (octreotide), a long-acting somatostatin receptor ligand, at a low dose that was gradually increased over the next few months based on how well she tolerated it and how her biochemical response changed. Regular follow-up lab tests showed that insulin-like growth factor-1 levels were steadily dropping toward the normal range. This showed that the excess growth hormone was being successfully suppressed. A follow-up MRI about a year into treatment showed a good response, with the adenoma getting smaller and cystic degeneration appearing in the tumor, which is what you would expect from somatostatin analog–mediated regression. This hormonal enhancement was accompanied by improved management of her metabolic comorbidities, including enhanced glycemic control, lowered blood pressure, and optimized lipid profiles, highlighting the close association between acromegaly and cardiometabolic complications. This case underscores the necessity of early recognition of acromegaly in patients primarily exhibiting metabolic disturbances and subtle physical manifestations, particularly when surgical intervention is not feasible. It also shows how effective somatostatin analogs can be as a powerful nonsurgical treatment that can help with biochemical control, tumor reduction, and overall metabolic health. In these cases, successful management depends on a personalized, multidisciplinary framework that includes regular endocrinological evaluations, hormonal monitoring, and periodic imaging. This is done to get the best disease control, reduce long-term complications, and improve quality of life.},
year = {2026}
}
TY - JOUR T1 - Medical Management of Acromegaly in a Middle-aged Woman with Pituitary Macroadenoma and Metabolic Comorbidities: A Case Report AU - Abdelrahman Shehata AU - Ayesha Aijaz AU - Ibrahim Ibrar AU - Abia Gouher AU - Muhammad Kamil Shahbaz AU - Mahir Jallo Y1 - 2026/03/19 PY - 2026 N1 - https://doi.org/10.11648/j.sdmed.20260101.14 DO - 10.11648/j.sdmed.20260101.14 T2 - Science Discovery Medicine JF - Science Discovery Medicine JO - Science Discovery Medicine SP - 19 EP - 23 PB - Science Publishing Group UR - https://doi.org/10.11648/j.sdmed.20260101.14 AB - A 62-year-old Iraqi woman exhibited progressive enlargement of her hands, feet, and facial features over several years, accompanied by poorly controlled type 2 diabetes mellitus, hypertension, and dyslipidemia—metabolic disorders that had become increasingly challenging to manage despite conventional treatment. These gradual physical changes, which are often very small in middle-aged and older people, eventually made doctors think that the person might have acromegaly. Biochemical testing confirmed the diagnosis by showing consistently high levels of growth hormone, no suppression on oral glucose tolerance testing, and insulin-like growth factor-1 concentrations that were much higher than normal for someone of the same age and sex. A macroadenoma measuring 14 × 12 × 9 mm was found on a pituitary magnetic resonance imaging scan. There was no suprasellar extension, optic chiasm compression, or visual field problems on formal testing. After a thorough discussion of treatment options, the patient opted against transsphenoidal surgery, citing personal preference and apprehensions about surgical risks, and instead chose to initiate primary medical treatment. She began taking Sandostatin LAR (octreotide), a long-acting somatostatin receptor ligand, at a low dose that was gradually increased over the next few months based on how well she tolerated it and how her biochemical response changed. Regular follow-up lab tests showed that insulin-like growth factor-1 levels were steadily dropping toward the normal range. This showed that the excess growth hormone was being successfully suppressed. A follow-up MRI about a year into treatment showed a good response, with the adenoma getting smaller and cystic degeneration appearing in the tumor, which is what you would expect from somatostatin analog–mediated regression. This hormonal enhancement was accompanied by improved management of her metabolic comorbidities, including enhanced glycemic control, lowered blood pressure, and optimized lipid profiles, highlighting the close association between acromegaly and cardiometabolic complications. This case underscores the necessity of early recognition of acromegaly in patients primarily exhibiting metabolic disturbances and subtle physical manifestations, particularly when surgical intervention is not feasible. It also shows how effective somatostatin analogs can be as a powerful nonsurgical treatment that can help with biochemical control, tumor reduction, and overall metabolic health. In these cases, successful management depends on a personalized, multidisciplinary framework that includes regular endocrinological evaluations, hormonal monitoring, and periodic imaging. This is done to get the best disease control, reduce long-term complications, and improve quality of life. VL - 1 IS - 1 ER -
College of Medicine, Gulf Medical University, Ajman, UAE
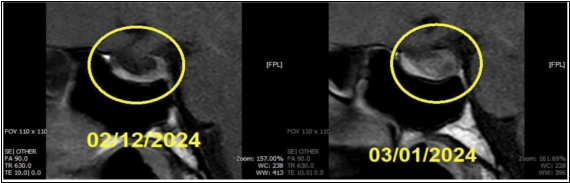
Figure 1. Sagittal T1-weighted MRI comparison of the pituitary gland showing a significant increase in the size of a sellar/suprasellar mass between February and March 2024.
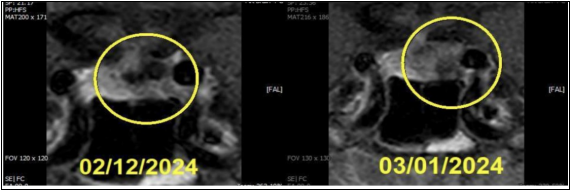
Figure 2. Coronal MRI views of the sellar region demonstrating interval growth of a soft tissue lesion with displacement of adjacent structures and narrowing of the suprasellar cistern.
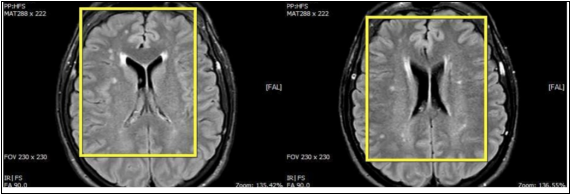
Figure 3. Axial FLAIR MRI sequences of the brain showing multiple hyperintense white matter lesions, which appear more numerous or prominent in the follow-up scan.
Information

