Abstract
This study aims to provide a descriptive analysis of the essential characteristics and demographic profiles, including age, weight, height, body mass index, marital status, and educational background in patients with chronic vulvar discomfort. The data were collected from the study DATRIV (Diagnostic Accuracy of Three Rings Vulvoscopy), which included 328 participants divided into four groups: normal vulva, impaired vulvar skin, primary vulvar distress/vulvodynia, and secondary discomfort caused by vulvar dermatoses. The clinical data collected from the study questionnaire were analyzed using statistical software such as StatSoft (Dell, Austin, TX, USA), Statistica 12 (TIBCO®, Palo Alto, CA, USA), and SPSS 20 (IBM, Armonk, NY, USA). The study was conducted with the approval of the Institutional Review Board of Polyclinic Harni, and all participants provided written informed consent. The findings from the DATRIV study shed light on several important aspects of chronic vulvar discomfort. They offered valuable insights into the demographic and reproductive characteristics of patients with chronic vulvar pain, specifically vulvar dermatosis. The study revealed that patients with vulvar dermatosis tended to be older, with a peak incidence in the 45-65 age range. They also had higher weight and BMI compared to other groups. There was a significant difference in the proportion of patients of reproductive age between the vulvar dermatosis group and other groups. Additionally, the vulvar dermatosis group had higher rates of marriage, births, and abortions and lower educational levels. The study's limitations included lacking patients younger than 16 years. Future research should aim to include a broader age range, including pediatric populations, to gain a more comprehensive understanding of vulvar dermatosis across different age groups. Further investigation is needed to uncover the underlying mechanisms and establish causal relationships, enhancing diagnosis, treatment, and support for individuals affected by vulvar dermatosis.
Keywords
Chronic Vulvar Discomfort, Vulvodynia, Vulvar Dermatosis, Demographics, DATRIV
1. Introduction
Chronic vulvar discomfort is a persistent pain condition that affects the vulvar region in women. Although there has been some exploration of the pain characteristics and underlying mechanisms, there remains a lack of research focusing on the essential characteristics and demographic data of patients with this condition
| [1] | International Association for the Study of Pain, Subcommittee on Taxonomy. Classification of chronic pain. Descriptions of chronic pain syndromes and definitions of pain terms. Pain Supplement 1986; 3: S1-S226. https://doi.org/10.1097/j.pain.0000000000001939 |
| [2] | Moyal-Barracco M, Lynch P. 2003 ISSVD terminology and classification vulvodynia: a historical perspective. J Reprod Med 2004; 49: 772-7. |
| [3] | Stockdale CK, Lawson HW. 2013 Vulvodynia Guideline update. J Low Genit Tract Dis 2014; 18: 93–100. https://doi.org/10.1097/LGT.0000000000000021 |
[1-3]
. Understanding the demographic patterns associated with chronic vulvar discomfort is crucial in identifying disease occurrence and prevalence patterns. Epidemiologists can use demographic data to identify prevalent risk factors within specific populations. Previous studies conducted in the USA have estimated the frequency of primary vulvar pain to be around 7-8% among women in the general adult population
| [4] | Harlow, BL, Kunitz, CG, Nguyen, RH, Rydell, SA, Turner, RM, MacLehose, RF. Prevalence of symptoms consistent with a diagnosis of vulvodynia: population-based estimates from 2 geographic regions. Am J Obstet Gynecol 2014; 210: 40 e1–8. https://doi.org/10.1016/j.ajog.2013.09.033 |
| [5] | Reed, BD, Harlow, SD, Sen, A, Legocki, LJ, Edwards, RM, Arato, N, et al. Prevalence and demographic characteristics of vulvodynia in a population-based sample. Am J Obstet Gynecol 2012; 206: 170 e1–9. https://doi.org/10.1016/j.ajog.2011.08.012 |
[4, 5]
. However, the prevalence of vulvar pain in European populations and clinical settings has received less attention
| [6] | Vieira-Baptista, P, Lima-Silva, J, Cavaco-Gomes, J, Beires, J. Prevalence of vulvodynia and risk factors for the condition in Portugal. Int J Gynaecol Obstet 2014; 127: 283–7. https://doi.org/10.1016/j.ijgo.2014.05.020 |
| [7] | Gomez, I, Coronado, PJ, Martin, CM, Alonso, R, Guisasola-Campa, FJ. Study on the prevalence and factors associated to vulvodynia in Spain. Eur J Obstet Gynecol Reprod Biol 2019; 240: 121–4. https://doi.org/10.1016/j.ejogrb.2019.06.005 |
| [8] | Edgardh, K, Abdelnoor, M. Longstanding vulval problems and entry dyspareunia among STD-clinic visitors in Oslo-results from a cross-sectional study. Int J STD AIDS 2003; 14: 796–9. https://doi.org/10.1258/095646203322556101 |
| [9] | Teigen, Per Kristen, Hagemann, Cecilie Therese, Fors, Egil Andreas, Stauri, Elisabeth, Hoffmann, Risa Lonnée and Schei, Berit. "Chronic vulvar pain in gynecological outpatients" Scandinavian Journal of Pain, 2023; 23 (1): 97-103. https://doi.org/10.1515/sjpain-2021-0223 |
[6-9]
.
Demographic data for patients with vulvodynia and vulvar dermatosis can vary, reflecting differences in the underlying conditions and their prevalence across different populations
. It is essential to acknowledge that the development and manifestation of primary/vulvodynia and secondary vulvar chronic discomfort /vulvar dermatosis are influenced by various factors, including age, weight, height, and BMI
| [12] | Hoftun GB, Romundstad PR, Rygg M. Factors associated with adolescent chronic nonspecific pain, chronic multisite pain, and chronic pain with high disability: the Young-HUNT Study 2008. J Pain. 2012; 13(9): 874–883. https://doi.org/10.1016/j.jpain.2012.06.001 |
| [13] | Yoo JJ, Cho NH, Lim SH, Kim HA. Relationships between body mass index, fat mass, muscle mass, and musculoskeletal pain in community residents. Arthritis Rheumatol. 2014; 66(12): 3511–3520. https://doi.org/10.1002/art.38861 |
[12, 13]
. Proposed etiologies or associated factors for these conditions include genetics, inflammation, frequent yeast infections, neuropathic pain, pelvic floor hypertonic dysfunctions, pelvic organ prolapse, hormone imbalances/hormonal contraceptives, high urine oxalates, and psychological disorders
| [14] | Groysman V. Vulvodynia: new concepts and review of the literature. Dermatol Clin. 2010; 28: 681-696. https://doi.org/10.1016/j.det.2010.07.002 |
| [15] | Falsetta ML, Foster DC, Bonham AD, Phipps RP. A review of the available clinical therapies for vulvodynia management and new data implicating proinflammatory mediators in pain elicitation. BJOG. 2017; 124: 210-218. https://doi.org/10.1111/1471-0528.14157 |
| [16] | Thomtén J, Lundahl R, Stigenberg K, Linton S. Fear avoidance and pain catastrophizing among women with sexual pain. Women’s Health (Lond). 2014; 10: 571-581. https://doi.org/10.2217/whe.14.51 |
[14-16]
. Additionally, individual variations and the diverse nature of these conditions can contribute to inconsistent findings in the existing literature.
Vulvodynia is commonly observed in women of reproductive age, typically between 18 and 40 years old. However, it can also occur in other age groups, including adolescents and postmenopausal women. The prevalence of vulvodynia varies, affecting approximately 4-16% of women in the general population. It can affect both nulliparous and parous women. The development of vulvodynia is not typically associated with specific demographic factors such as race or ethnicity. However, certain factors, such as a history of recurrent yeast infections, previous vaginal infections, a history of sexual abuse, or a family history of chronic pain conditions, may increase the risk of developing vulvodynia
| [5] | Reed, BD, Harlow, SD, Sen, A, Legocki, LJ, Edwards, RM, Arato, N, et al. Prevalence and demographic characteristics of vulvodynia in a population-based sample. Am J Obstet Gynecol 2012; 206: 170 e1–9. https://doi.org/10.1016/j.ajog.2011.08.012 |
| [17] | Vasileva P, Strashilov SA, Yordanov AD. Aetiology, diagnosis, and clinical management of vulvodynia. Prz Menopauzalny. 2020 Mar; 19(1): 44-48. Epub 2020 Apr 27. PMID: 32699543; PMCID: PMC7258372. https://doi.org/10.5114/pm.2020.95337 |
[5, 17]
.
The age distribution of patients with vulvar dermatosis can vary depending on the specific condition. Traditional teaching suggests that vulvar dermatosis has a bimodal onset in prepubertal children and postmenopausal women
| [18] | Cooper SM, Baldo AM, Wojnarowska F. The association of lichen sclerosus and erosive lichen planus of the vulva with autoimmune disease: a case-control study. Arch Dermatol, 144 (11) (2008), pp. 1432-1435. https://doi.org/10.1001/archderm.144.11.1432 |
| [19] | Fistarol SK, Itin PH. Diagnosis and treatment of lichen sclerosus: an update. Am J Clin Dermatol, 14 (1) (2013), pp. 27-47. https://doi.org/10.1007/s40257-012-0006-4 |
| [20] | Schlosser BJ, Mirowski GW. Lichen sclerosus and lichen planus in women and girls. Clin Obstet Gynecol, 58 (1) (2015), pp. 125-142. https://doi.org/10.1097/GRF.0000000000000090 |
[18-20]
. In most studies, the majority of women with vulvar dermatosis (79%) were between the ages of 45 and 65 years, with an average age of 50.8 years. Sixteen percent of patients with lichen sclerosus (LS) were 18 to 44 years old. In pediatric patients (aged 0-17 years), the prevalence of the disease was 0.01%
| [21] | Melnick LE, Steuer AB, Bieber AK, Wong PW, Pomeranz MK. Lichen sclerosus among women in the United States. Int J Womens Dermatol. 2020 May 8; 6(4): 260-262. PMID: 33015282; PMCID: PMC7522895. https://doi.org/10.1016/j.ijwd.2020.05.001 |
[21]
. One study from London reported that approximately 20% of patients developed LS during their reproductive years
| [22] | Trokoudes D, Lewis FM. Lichen sclerosus - the course during pregnancy and effect on delivery. J Eur Acad Dermatol Venereol, 33 (12) (2019), pp. e466-e468. https://doi.org/10.1111/jdv.15788 |
[22]
, while another study in Beijing found that 75.2% of their sample of 129 women developed LS during the childbearing period
.
Limited research has been conducted to investigate weight, height, and BMI differences between patients with chronic vulvar discomfort and those without. Some studies suggest a potentially higher prevalence of vulvar discomfort symptoms, such as atopic dermatitis or atopic eczema, among individuals who are overweight or obese. This association may be attributed to chronic inflammation resulting from induced immune dysfunction. However, the relationship between weight, height, BMI, and chronic vulvar discomfort is not fully understood
| [24] | Powell, A. M., Sarria, I. & Goje, O. Role of Obesity in Recurrent Vulvovaginal Symptoms and Disease. Curr Infect Dis Rep 25, 1–6 (2023). https://doi.org/10.1007/s11908-022-00793-2 |
| [25] | Tan IF, AW. Chapter 31 - Obesity and chronic pelvic pain, Editor(s): Tahir A. Mahmood, Sabaratnam Arulkumaran, Frank A. Chervenak, Obesity and Gynecology (Second Edition), Elsevier, 2020: 281-291, ISBN 9780128179192, https://doi.org/10.1016/B978-0-12-817919-2.00031-0 |
[24, 25]
. It is important to note that these findings are not consistently reported in all studies, and further research is needed to establish a clear association, if any, between weight, height, BMI, and chronic vulvar discomfort
| [26] | Okifuji A, Hare BD. The association between chronic pain and obesity. J Pain Res. 2015 Jul 14; 8: 399-408. PMID: 26203274; PMCID: PMC4508090. https://doi.org/10.2147/JPR.S55598 |
| [27] | Pudalov LR, Krause SJ, Heinberg LJ, Hogue O. Refractory Chronic Pain and Obesity: Promising Implications for Multidisciplinary Pain Rehabilitation, Pain Medicine, 2021; 22 (10): 2290–2297, https://doi.org/10.1093/pm/pnab055 |
[26, 27]
.
Similarly, the available research is limited and inconsistent when comparing weight, height, and BMI between patients with vulvodynia and vulvar dermatosis. Some studies suggest a potential association between higher BMI and vulvodynia, while others do not find a significant relationship. However, the evidence is insufficient to draw definitive conclusions about weight, height, and BMI differences in vulvar dermatosis. Further research is needed to explore these factors and their potential role in developing and manifesting vulvar discomfort conditions.
The impact of chronic vulvar discomfort on marital status, births, and abortions has been understudied, and there is limited research examining the relationship between these demographic factors and chronic vulvar pain. Marital status is influenced by various personal, social, and cultural factors that are independent of vulvar discomfort. Similarly, the influence of chronic vulvar discomfort on births or abortions requires further investigation to establish any potential associations.
However, some studies have provided insights into the demographic characteristics of women with chronic vulvar pain. For example, among women with chronic vulvar pain, a high proportion (75%) were married or in a marriage-like relationship
| [28] | Bachmann GA, Rosen R, Arnold LD, Burd I, Rhoads GG, Leiblum SR, Avis N. Chronic vulvar and other gynecologic pain: prevalence and characteristics in a self-reported survey. J Reprod Med. 2006 Jan; 51(1): 3-9. |
[28]
. Women presenting with vulvodynia are typically in stable, long-term relationships, and they have often experienced the pain for several years before receiving a diagnosis
. The average age of these women was reported to be thirty-eight, and 55% were married, while 54% had not experienced a pregnancy
| [30] | Sadownik LA. Clinical profile of vulvodynia patients. A prospective study of 300 patients. J Reprod Med. 2000 Aug; 45(8): 679-84. |
[30]
.
In the case of vulvar dermatosis, most of the patients were reported to be married (91.92%), housewives (82.88%), and illiterate (49.61%) women
| [31] | Shaik H, Konala S, Kolalapudi SA, Alluri R, Godha V, Navya B. Clinical and Demographic Patterns of Vulval Dermatoses and Their Impact on Quality of Life. Indian Dermatol Online J. 2022 Dec 14; 14(1): 44-49. https://doi.org/10.4103/idoj.idoj_339_22 |
[31]
. These findings provide some preliminary insights into the demographic characteristics of individuals with chronic vulvar dermatosis, but further research is needed to gain a comprehensive understanding of the relationship between chronic vulvar discomfort and marital status, as well as the influence on births and abortions.
The research on the differences in education between patients with vulvodynia and vulvar dermatosis is limited, and there is insufficient data to draw definitive conclusions. Some studies have indicated that care seekers for vulvodynia were more likely to have a college education
| [32] | Bond JC, Harlow BL, White KO. Care Seeking for Chronic Vulvar Pain Among a Large, Population-Based Sample of Reproductive-Aged Women. J Womens Health (Larchmt). 2022 Apr; 31(4): 513-520. https://doi.org/10.1089/jwh.2021.0086 |
| [33] | Joypaul S, Kelly F, McMillan SS, King MA. Multi-disciplinary interventions for chronic pain involving education: A systematic review. PLOS. 2019, https://doi.org/10.1371/journal.pone.0223306 |
[32, 33]
, with approximately 60% having a college or graduate degree
| [28] | Bachmann GA, Rosen R, Arnold LD, Burd I, Rhoads GG, Leiblum SR, Avis N. Chronic vulvar and other gynecologic pain: prevalence and characteristics in a self-reported survey. J Reprod Med. 2006 Jan; 51(1): 3-9. |
[28]
. However, no significant differences in pain-related disability were identified between higher and lower-educated participants
| [34] | Bilterys T, Kregel J, Nijs J, Meeus M, Danneels L, Cagnie B, Van Looveren E, Malfliet A. Influence of education level on the effectiveness of pain neuroscience education: A secondary analysis of a randomized controlled trial. Musculoskelet Sci Pract. 2022; 57: 102494. https://doi.org/10.1016/j.msksp.2021.102494 |
| [35] | Geneen, L. J., Martin, D. J., Adams, N. et al. Effects of education to facilitate knowledge about chronic pain for adults: a systematic review with meta-analysis. Syst Rev. 2015; 132(4): 132. https://doi.org/10.1186/s13643-015-0120-5 |
[34, 35]
.
Given that vulvodynia can affect women of various ages and backgrounds, it is expected that individuals with vulvodynia will have diverse educational levels. One study reported that 72% of women with vulvodynia had postsecondary education
| [30] | Sadownik LA. Clinical profile of vulvodynia patients. A prospective study of 300 patients. J Reprod Med. 2000 Aug; 45(8): 679-84. |
[30]
. However, available studies do not typically consider education as a primary variable of interest concerning these conditions.
There is no specific indication or evidence to suggest a correlation between educational attainment and the development or prevalence of vulvodynia. Similarly, there is no established association between educational level and the development of vulvar dermatoses such as lichen sclerosus, lichen planus, or other related conditions. These conditions can occur in individuals from different academic backgrounds.
Recognizing that educational attainment is influenced by various social, cultural, and economic factors unrelated to vulvodynia or vulvar dermatosis is essential. The impact of chronic vulvar discomfort on education can vary depending on the severity of symptoms, pain management strategies, and individual coping mechanisms. Some individuals with chronic pain conditions may experience challenges in terms of concentration, attendance, or participation in educational activities. However, the extent of these challenges is highly subjective and can vary significantly between individuals.
Future research should prioritize gathering more comprehensive data on the demographic characteristics of individuals with chronic vulvar discomfort and their potential associations. Understanding the demographic profiles of affected individuals is crucial for tailoring treatment approaches, identifying possible risk factors, and developing appropriate support services.
The primary objective of this study is to provide a descriptive analysis of the basic characteristics and demographic data of patients with chronic vulvar discomfort. A thorough review of existing literature, clinical records, and patient databases from the DATRIV study (Diagnostic Accuracy of Three Rings Vulvoscopy) was conducted to gather relevant information. The study examined age, weight, height, reproductive factors, marital status, and educational background. These findings have the potential to contribute to a better understanding of the demographic profile of individuals with chronic vulvar discomfort and can inform targeted interventions and support services.
2. Methods
The DATRIV study (Diagnostic Accuracy of Three Rings Vulvoscopy) aimed to improve the diagnosis and treatment of vulvar discomfort and establish standard outcome measures in vulvoscopy, particularly Three Rings Vulvoscopy (TRIV)
| [36] | Harni V, Babic D, Hadzavdic S, Barisic D. Diagnostic Accuracy of the Vulvoscopy Index for Detection of Vulvar Dermatosis (DATRIV Study, Part 1). Journal of Gynecology and Obstetrics 2022; Vol. 10, No. 1, 39-47. https://doi.org/10.11648.j.jgo.20221001.16 |
| [37] | Harni V, Babic D, Hadzavdic S, Barisic D. Clinical Value of the N-S-P Scheme for Detection of Vulvar Dermatosis (DATRIV Study, Part 2). Journal of Gynecology and Obstetrics 2022; Vol. 10, No. 3, 159-166. https://doi.org/10.11648.j.jgo.20221003.11 |
[36, 37]
.
Lesions observed during the study were categorized based on recommended general principles
| [38] | Bornstein J, Sideri M, Tatti S, Walker P, Prendiwille W, Haefner HK. 2011 Terminology of the Vulva of the International Federation for Cervical Pathology and Colposcopy. J Lower Genit Tract Dis 2012; 16: 290-5. https://doi.org/10.1097/LGT.0b013e31825934c7 |
| [39] | van Beurden M, van der Vange N, de Craen AJM, Tjong-A-Hung SP, ten Kate FJW, ter Schegget J, et al. Normal findings in vulvar examination and vulvoscopy. J Br Obstet Gynaecol 1997; 104: 320-4. https://doi.org/10.1111/j.1471-0528.1997.tb11461.x |
[38, 39]
. Dermatological lesions with secondary morphological presentation were termed "specific lesions"
| [40] | Byrne MA, Walker MM, Leonard J, Pryce D, Taylor-Robinson D. Recognising covert disease in women with chronic vulval symptoms attending an STD clinic: value of detailed examination including colposcopy. Genitourin Med 1989; 65: 46-9. https://doi.org/10.1136/sti.65.1.46 |
| [41] | Audisio T, Zarazaga J, Vainer O. A Classification of Vulvoscopic Findings for Clinical Diagnosis. J Lower Genit Tract Dis 1999; 3: 7-18. https://doi.org/10.1046/j.1526-0976.1999.08079.x. |
[40, 41]
. Their localization was described concerning the three vulvar rings
| [42] | Harni V, Babic D, Barisic D. "Three Rings Vulvoscopy" – A New Approach to the Vulva. Gynaecol Perinatol 2015; 24: 37-45. |
| [43] | Harni V, Babic D, Barisic D. "Three Rings Vulvoscopy" – A New Approach to the Vulva. Chapter in Watson L (ed.) Cryosurgery and Colposcopy: Practices, Outcomes, and Potential Complications. New York, Nova Science Publishers Inc; 2016. ISBN: 978-1-63484-507-6. |
[42, 43]
.
The study distinguished four groups of patients based on their history, ISSVD Vulvodynia Pattern Questionnaire results, and clinical examination. Asymptomatic participants were divided into a "normal vulva" group and an "impaired vulvar skin" group. Patients with chronic vulvar discomfort were categorized into primary vulvar pain/vulvodynia and secondary discomfort caused by vulvar dermatosis.
Regardless of the vulvar lesions observed, vulvodynia was diagnosed based on Friedrich's criteria
. Diagnosing vulvar dermatosis involved identifying specific dermatological lesions with secondary morphological presentations and evaluating the presence and distribution of nonspecific lesions across the three vulvar rings.
The study was conducted at the Polyclinic Harni in Zagreb, Croatia, between December 1, 2011, and December 31, 2016. It included both symptomatic and asymptomatic patients, with exclusion criteria related to certain vulvar conditions, incomplete medical records, and protocol violations.
TRIV and vulvar biopsy with histopathology were performed in all four patient groups. Vulvar biopsies were conducted as part of routine clinical care for symptomatic patients, while asymptomatic participants were recruited from those undergoing planned labiaplasty.
The study analyzed basic characteristics and demographic data as secondary outcome measures. These details provide a comprehensive understanding of the DATRIV study's objectives, patient groups, diagnostic interventions, and data collection methods. The study aimed to contribute to diagnosing and treating vulvar discomfort while also examining the demographic and clinical characteristics of the participants.
Different statistical tests were employed to analyze qualitative and quantitative variables, considering their nature and distribution.
The chi-squared test was utilized for qualitative variables (categorical variables), with Yates correction applied for 2x2 contingency tables and Fisher's exact test used for small sample sizes. The t-test for proportions was applied to assess quantitative variables (continuous variables) with a confirmed normal distribution, and descriptive statistics such as the arithmetic mean and standard deviation were calculated. Variance analysis (ANOVA) was performed to compare means among multiple groups, and the post hoc Tukey HSD test was used to identify specific differences between groups. When comparing means between two groups, the t-test was employed.
Table 1. Age of patients with and without vulvar discomfort in the DATRIV Study.
Age | Normal vulva (N=82) | Impaired vulvar skin (N=82) | Vulvodynia (N=82) | Vulvar dermatosis (N=82) |
Mean (years) | 34.2 | 34.4 | 34.2 | 51.** |
| SD | 10.0 | 9.4 | 10.0 | 16.2 |
Median (years) | 34 | 32.5 | 34 | 53 ** |
| SD | 18-63 | 18-66 | 18-63 | 16-83 |
Reproductive age | 77 (93.9%) | 79 (96.3%) | 76 (92.7%) | 36 (43.9%) ** |
Age >65 years | 0 (0%) | 1 (1.2 "%) | 0 (0%) | 15 (18.3%) ** |
Hormone replacement therapy | 1 (1.2%) | 0 (0%) | 1 (1.2%) | 1 (1.2%) |
Statistics | ANOVA (Mean age) | Kruskal-Wallis ANOVA (Median age) | Hi-square test (Reproductive age) (Age >65 years) |
Vulvar Dermatosis vs. Normal vulva | p = 0.0000 ** | p = 0.0000 ** | p = 0.0000 ** |
Vulvar Dermatosis vs. Impaired Vulvar Skin | p = 0.0000 ** | p = 0.0000 ** | p = 0.0000 ** |
Vulvar Dermatosis vs. Vulvodynia | p = 0.0000 ** | p = 0.0000 ** | p = 0.0000 ** |
Nonparametric tests were used for quantitative variables that did not follow a normal distribution. The Kruskal-Wallis ANOVA was utilized to test differences among several groups, and the Mann-Whitney U test was applied to compare differences between the two groups. All statistical analyses were conducted using the Statistical Package 12.0 on a personal computer (PC).
All participants were informed that their participation in the study was voluntary. They were allowed to decline participation in the questionnaire if they chose to do so. Patients who underwent vulvoscopy and vulvar biopsy provided written informed consent. That indicates that they were fully informed about the nature of the procedures, potential risks, and benefits and voluntarily agreed to participate after understanding the information provided.
The study obtained ethical permission from the Institutional Review Board of Polyclinic Harni. It was assigned an Ethical Approval Number (20111201001), indicating that it met the necessary ethical standards and guidelines set by the review board.
The DATRIV study was registered on ClinicalTrials.gov with the identifier NCT02732145. Registering the survey on this platform helps ensure transparency and informs the research community and the public about the study's purpose, design, and outcomes.
These ethical measures demonstrate that the study followed ethical guidelines and safeguards to protect the rights and welfare of the participants. Informed consent and voluntary participation are essential ethical principles in research studies, and obtaining ethical approval and registering the study further ensures adherence to ethical standards and enhances transparency in research practices.
3. Results
3.1. Age, Reproductive Age, Age >65 Years, HRT
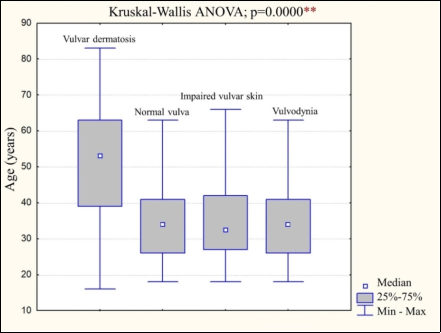
The analysis revealed that patients with chronic vulvar discomfort encompassed a diverse demographic profile. Age distribution ranged from adolescents to older adults, with a peak incidence observed in women aged 34.2-51.1 years (
Table 1). Patients with normal vulva, impaired vulvar skin, and vulvodynia have similar mean ages, around 34 years, with a range of 18 to 66 years. That suggests no significant difference in age among these three groups.
Patients with vulvar dermatosis are reported to be statistically significantly older than subjects from the other groups. The statistical analysis likely determined that the age difference between patients with vulvar dermatosis and the different groups is statistically significant (
Figure 1).
Figure 1. Age of patients with and without vulvar discomfort in the DATRIV Study.
3.2. Weight, Height, and BMI
Post-hoc analysis (Tukey HSD) found that the vulvar dermatosis group statistically differed significantly from other groups, while these three mutually did not differ. Patients in the group of vulvar dermatoses were considerably more severe than others and had substantially higher BMIs.
The difference in the height of the patients was at the limit of statistical significance. The difference in the height of the patients from the normal vulva and vulvodynia groups was borderline significant (p = 0.0606). At the same time, there was no difference among the other groups.
Table 2. Weight, height and BMI – body mass index in patients with and without vulvar discomfort in the DATRIV Study.
Weight Height BMI | Normal vulva (N=82) | Impaired vulvar skin (N=82) | Vulvodynia (N=82) | Vulvar dermatosis (N=82) |
Weight (kg) | 61.9 | 63.3 | 61.1 | 71.3 ** |
| SD | 8.3 | 10.9 | 9.2 | 12.0 |
Height (cm) | 169.1 | 168.7 | 166.7 | 167.5 |
| SD | 6.0 | 6.3 | 6.7 | 5.7 |
BMI (kg/cm) | 21.6 | 22,3 | 22.0 | 25.4 ** |
| SD | 2.5 | 3.6 | 2.9 | 4.1 |
Statistics | ANOVA (Weight / BMI) |
Vulvar Dermatosis vs. Normal vulva | p = 0.0000 ** |
Vulvar Dermatosis vs. Impaired Vulvar Skin | p = 0.0000 ** |
Vulvar Dermatosis vs. Vulvodynia | p = 0.0000 ** |
3.3. Marital Status, Births and Abortions
There were six divorced women and nine widows in the marital status category. This number was too small for the diagnosis group, so they were linked to the married category, and the pattern was tested compared with unmarried participants. The test was repeated after excluding these patients (divorced and widows). In each of these combinations, the result of the analysis was the same: in the vulvar dermatosis group, there were statistically significantly more married women than in the other three groups (
Table 3.).
The testing proved that there is a statistically significant difference in the number of births among the groups of test subjects. Patients with vulvar dermatosis had more births than others (p = 0.0000).
Table 3. Marital status, births and abortions in patients with and without vulvar discomfort in the DATRIV Study.
Marital status Births Abortions | Normal vulva (N=82) | Impaired vulvar skin (N=82) | Vulvodynia (N=82) | Vulvar dermatosis (N=82) |
Married | 44 (53.7%) | 39 (47.6%) | 44 (53.7%) | 69 (84.2%) ** |
Births | 0 | 49 (59.8%) | 52 (63.4%) | 44 (53.7%) | 17 (20.7%) ** |
| 1 | 13 (15.8%) | 11 (13.4%) | 17 (20.7%) | 22 (26.9%) |
| 2 | 14 (17.1%) | 15 (18.3%) | 15 (18.3%) | 31 (37.8%) |
| ≥3 | 6 (7.3%) | 4 (4.9%) | 6 /7.3%) | 12 (14.6%) |
Interval since last birth (women who have given birth) | 33/82 | 30/82 | 38/82 | 65/82 |
| Median (years) | 8 | 6 | 8 | 22 |
| Range (years) | 1-34 | 2-28 | 1-29 | 1-58 |
Abortions | 0 | 74 (90.3%) | 75 (91.4%) | 67 (81.7%) | 53 (64.6%) ** |
| 1 | 6 (7.3%) | 4 (4.9) | 10 (12.2%) | 14 (17.1%) |
| ≥2 | 2 (2.4%) | 3 (3.7%) | 5 (6.1%) | 15 (18.3%) |
In parallel, it was assessed whether the patients of individual groups differed by whether they had given birth at all or not. Again, it was proven that a higher proportion of patients from the group of vulvar dermatoses gave birth than from other groups. Patients with other diagnoses did not differ from each other on this issue.
In patients with vulvar dermatosis, an average of 22 years has passed since their last delivery, while the patients of the other groups last gave birth an average of 6 to 8 years ago. Only those patients who gave birth were included in this analysis. The difference is statistically significant, which is logical because the patients from the vulvar dermatosis group were significantly older than the others.
Only three patients had three abortions each, so in the analysis, they are included in category two and more abortions. Patients from the vulvar dermatosis group had statistically significantly more abortions than patients from other groups. The different groups did not differ in the number of abortions. Suppose the patients of all groups are compared according to whether they had an abortion or not, among those who had an abortion. In that case, there are statistically significantly more of those with vulvar dermatosis.
3.4. Country of Birth and Educational Background
There was no statistically significant association between the country of birth and the occurrence of vulvodynia or vulvar dermatosis (
Table 4.).
Table 4. Country of birth and education level of patients with and without vulvar discomfort in the DATRIV Study.
Age | Normal vulva (N=82) | Impaired vulvar skin (N=82) | Vulvodynia (N=82) | Vulvar dermatosis (N=82) |
Country of birth | Native country | 68 (82.9%) | 62 (75.6%) | 68 (82.9%) | 61 (74.4%) |
| Foreign country | 14 (17.1%) | 20 (24.4%) | 14 (17.1%) | 21 (25.6%) |
Education | ≤12 years | 30 (36.6%) | 24 (29.3%) | 30 (36.6%) | 40 (48.8%) * |
| >12 years | 52 (63.4%) | 58 (70.7%) | 52 (63.4%) | 42 (51.2%) |
There were no statistically significant differences in the education of female patients. The table shows fewer patients with more than 12 years of education in the vulvar dermatosis group than in the other groups with the same number of patients. Therefore, a chi-square test was performed between the vulvar dermatosis group and all others. In that case, a statistically significant difference was obtained at the p = 0.0180 (chi-square test), which means that the patients of the vulvar dermatosis group are less educated than the others (
Table 4).
4. Discussion
The results of the presented study provide valuable insights into the relationship between age, reproductive factors, and educational status among patients with chronic vulvar discomfort. The analysis demonstrated that patients with chronic vulvar discomfort exhibit diverse demographics.
The age distribution ranged from adolescents to older adults, with a peak incidence observed in women aged 34.2-51.1 years. Interestingly, patients with normal vulva, impaired vulvar skin, and vulvodynia showed similar mean ages, around 34 years, with an age range of 18 to 66 years. These findings suggest no significant difference in age among these three groups. Previously, it was described that vulvodynia affects women of every age, reproductive period, and ethnicity
| [17] | Vasileva P, Strashilov SA, Yordanov AD. Aetiology, diagnosis, and clinical management of vulvodynia. Prz Menopauzalny. 2020 Mar; 19(1): 44-48. Epub 2020 Apr 27. PMID: 32699543; PMCID: PMC7258372. https://doi.org/10.5114/pm.2020.95337 |
[17]
. The average age of the onset of vulvodynia was approximately 30 years, while it varies extensively between 6 and 70 years of age
| [5] | Reed, BD, Harlow, SD, Sen, A, Legocki, LJ, Edwards, RM, Arato, N, et al. Prevalence and demographic characteristics of vulvodynia in a population-based sample. Am J Obstet Gynecol 2012; 206: 170 e1–9. https://doi.org/10.1016/j.ajog.2011.08.012 |
[5]
.
In contrast, the study findings indicate that patients with vulvar dermatosis are significantly older than patients in other groups. The observed differences in age between patients with vulvar dermatosis and the comparison groups reached statistical significance at a shallow p-value level of p < 0.0000. That contrasts with previous data, which showed that the most common age of patients with vulvar dermatosis was 31-40 years
| [31] | Shaik H, Konala S, Kolalapudi SA, Alluri R, Godha V, Navya B. Clinical and Demographic Patterns of Vulval Dermatoses and Their Impact on Quality of Life. Indian Dermatol Online J. 2022 Dec 14; 14(1): 44-49. https://doi.org/10.4103/idoj.idoj_339_22 |
[31]
. However, this corresponds to other authors who described an average data set between ages 45 and 65
| [21] | Melnick LE, Steuer AB, Bieber AK, Wong PW, Pomeranz MK. Lichen sclerosus among women in the United States. Int J Womens Dermatol. 2020 May 8; 6(4): 260-262. PMID: 33015282; PMCID: PMC7522895. https://doi.org/10.1016/j.ijwd.2020.05.001 |
[21]
.
Importantly, this study highlights age as a differentiating factor between patients with vulvar dermatosis and the other groups, indicating that patients with vulvar dermatosis tend to be older than those in the comparison groups. These findings suggest that the age difference between these groups is doubtful to have occurred by chance alone, underscoring the significance of age as a potential risk factor or characteristic associated with vulvar dermatosis.
Considering that the study was conducted in a gynecological clinic and the youngest patient was 16 years old, it is understandable that the study may have limitations in accurately assessing the age of patients with vulvar discomfort, particularly regarding the incidence of vulvar dermatosis in childhood.
Vulvar dermatosis can indeed have two incidence peaks, with the first peak occurring in childhood
| [18] | Cooper SM, Baldo AM, Wojnarowska F. The association of lichen sclerosus and erosive lichen planus of the vulva with autoimmune disease: a case-control study. Arch Dermatol, 144 (11) (2008), pp. 1432-1435. https://doi.org/10.1001/archderm.144.11.1432 |
| [19] | Fistarol SK, Itin PH. Diagnosis and treatment of lichen sclerosus: an update. Am J Clin Dermatol, 14 (1) (2013), pp. 27-47. https://doi.org/10.1007/s40257-012-0006-4 |
| [20] | Schlosser BJ, Mirowski GW. Lichen sclerosus and lichen planus in women and girls. Clin Obstet Gynecol, 58 (1) (2015), pp. 125-142. https://doi.org/10.1097/GRF.0000000000000090 |
[18-20]
. By excluding younger patients below the age of 16, the study may have missed capturing cases of vulvar dermatosis in this age group. Consequently, the findings may not fully represent the accurate age distribution of patients with vulvar dermatosis.
It is essential to recognize the limitations of a study and acknowledge the potential impact on the generalizability of the findings. In the case of the DATRIV study, excluding patients under 16 may have limited the assessment of vulvar dermatosis in younger age groups. Future studies targeting a broader age range, including pediatric populations, would be valuable in providing a more comprehensive understanding of the incidence and characteristics of vulvar dermatosis across different age groups. Understanding these age-related differences can contribute to a better understanding of the condition and its potential underlying causes or risk factors.
Regarding reproductive factors, the study found a significant difference in the proportion of patients of reproductive age between the vulvar dermatosis group and other groups. Over 90% of patients in the different groups were of reproductive age, while only 43.9% of the vulvar dermatosis group patients fell within this age range. This difference reached statistical significance. Similarly, a higher proportion of subjects with vulvar dermatosis were postmenopausal compared to the other groups.
Among the vulvar dermatosis group patients, 18.3% (15 out of 82) were older than 65. In contrast, no patients older than 65 were in the other groups, except one in the impaired vulvar skin group. This age difference was statistically significant, with a p-value of 0.0000.
It is important to note that the number of patients receiving hormone replacement therapy (HRT) in the DATRIV study was insufficient for meaningful analysis, as only three out of 328 patients received HRT.
Furthermore, the analysis revealed a significant difference in weight and BMI between patients in distinct groups. Further post-hoc analysis using the Tukey HSD test indicated that the vulvar dermatosis group exhibited a significant difference compared to the other groups. In contrast, no significant differences were found between the normal vulva, impaired vulvar skin, and vulvodynia groups. Specifically, patients with vulvar dermatosis exhibit significantly higher BMI compared to other groups, which is interesting concerning the fact that women suffering from chronic vulvar discomfort with a higher BMI are less likely to seek medical help
| [32] | Bond JC, Harlow BL, White KO. Care Seeking for Chronic Vulvar Pain Among a Large, Population-Based Sample of Reproductive-Aged Women. J Womens Health (Larchmt). 2022 Apr; 31(4): 513-520. https://doi.org/10.1089/jwh.2021.0086 |
[32]
.
The height difference among groups was at the limit of statistical significance but did not show substantial variation. Regarding height, the difference among the patient groups was at the limit of statistical significance. The difference in the height of the patients from the normal vulva and vulvodynia groups was borderline significant (p = 0.0606). However, no significant differences were observed among the remaining groups.
These findings suggest a potential association between weight/BMI and vulvar dermatosis, indicating the need for further investigation into body composition's role in the condition's development or progression.
Interpreting these findings cautiously and considering the study's potential limitations is essential. Further research may be necessary to comprehensively explore the associations between weight, BMI, height, and different vulvar conditions.
The study uncovers a significant difference in marital status and the number of births among the groups, with patients with vulvar dermatosis more likely to be married and have a higher number of births compared to other groups. That aligns with findings from different studies, which also observed that most of their patients with vulvar dermatosis were married and housewives
| [31] | Shaik H, Konala S, Kolalapudi SA, Alluri R, Godha V, Navya B. Clinical and Demographic Patterns of Vulval Dermatoses and Their Impact on Quality of Life. Indian Dermatol Online J. 2022 Dec 14; 14(1): 44-49. https://doi.org/10.4103/idoj.idoj_339_22 |
[31]
.
However, findings from the literature regarding the relationship between marital status and vulvodynia vary. Some authors suggest that patients with vulvodynia are typically in stable, long-term relationships, and marriage may provide a protective factor against depression and anxiety
| [46] | Jantos M, Burns NR. Vulvodynia. Development of a psychosexual profile. J Reprod Med. 2007 Jan; 52(1): 63-71. |
| [29] | Reed BD, Crawford S, Couper M, et al. Pain at the Vulvar Vestibule: A Web-Based Survey. J Low Genit Tract Dis 2004; 8: 48-57. https://doi.org/10.1097/00128360-200401000-00011 |
[46, 29]
. Conversely, other studies have reported a higher prevalence of unmarried women among patients with vulvodynia
| [47] | Patla G, Mazur-Bialy AI, Humaj-Grysztar M, Bonior J. Chronic Vulvar Pain and Health-Related Quality of Life in Women with Vulvodynia. Life (Basel). 2023 Jan 24; 13(2): 328. https://doi.org/10.3390/life13020328 |
[47]
.
The study suggests a significant association between parity and chronic vulvar discomfort, particularly in patients with vulvar dermatosis. Specifically, patients with vulvar dermatosis were found to have a higher number of births compared to other groups in the study (p = 0.0000). Several studies have explored the relationship between parity and chronic vulvar discomfort. Some findings suggest that higher parity may be associated with an increased risk of developing chronic vulvar discomfort, while others have not found a significant association
| [48] | Driul L, Bertozzi S, Londero AP, Fruscalzo A, Rusalen A, Marchesoni D, Di Benedetto P. Risk factors for chronic pelvic pain in a cohort of primipara and secondipara at one year after delivery: association of chronic pelvic pain with autoimmune pathologies. Minerva Ginecol. 2011 Apr; 63(2): 181-7. |
[48]
.
One potential explanation for this association is the trauma experienced during childbirth, especially vaginal delivery, which can result in injury or irritation to the pelvic floor muscles and nerves. Such trauma may contribute to the development of chronic vulvar discomfort. Additionally, hormonal changes and alterations in pelvic anatomy associated with pregnancy and childbirth could also play a role in the onset of vulvar discomfort.
These findings underscore the importance of considering parity as a potential risk factor in assessing and managing chronic vulvar discomfort. Further research is warranted to better understand this association's mechanisms and explore potential preventive and therapeutic interventions.
In patients with vulvar dermatosis, an average of 22 years has passed since their last delivery, while the patients of the other groups last gave birth an average of 6 to 8 years ago. The difference is statistically significant, which is logical because the patients from the vulvar dermatosis group were significantly older than the others.
Patients from the vulvar dermatosis group had statistically significantly more abortions than patients from other groups. The different groups did not differ in the number of abortions. Suppose the patients of all groups are compared according to whether they had an abortion or not, among those who had an abortion. In that case, there are statistically significantly more of those with vulvar dermatosis.
There may be associations between the country of birth and chronic vulvar discomfort, as various factors such as cultural practices, environmental influences, access to healthcare, and genetic predispositions can differ among populations from different regions or countries, but this study does not detect a significant association.
Moreover, specific research directly investigating the association between country of birth and chronic vulvar discomfort appears limited. Studies focusing on the epidemiology and risk factors of vulvar discomfort often include demographic variables such as age, ethnicity, and socioeconomic status, but the country of birth may not always be specifically examined.
The study uncovered a notable difference in educational attainment between the group with vulvar dermatosis and the other groups, indicating that patients with vulvar dermatosis tended to have lower levels of education. This observation suggests a potential link between educational status and vulvar dermatosis, prompting the need for further investigation into the underlying factors shaping this association.
However, it's important to note that findings regarding the relationship between education and vulvar dermatosis vary across different studies. Some studies have reported that a majority of patients with vulvar dermatosis were illiterate
| [31] | Shaik H, Konala S, Kolalapudi SA, Alluri R, Godha V, Navya B. Clinical and Demographic Patterns of Vulval Dermatoses and Their Impact on Quality of Life. Indian Dermatol Online J. 2022 Dec 14; 14(1): 44-49. https://doi.org/10.4103/idoj.idoj_339_22 |
[31]
, while others have found that care seekers with chronic vulvar pain were more likely to have a university education
| [32] | Bond JC, Harlow BL, White KO. Care Seeking for Chronic Vulvar Pain Among a Large, Population-Based Sample of Reproductive-Aged Women. J Womens Health (Larchmt). 2022 Apr; 31(4): 513-520. https://doi.org/10.1089/jwh.2021.0086 |
[32]
. Conversely, certain studies have failed to identify any significant differences in educational levels concerning vulvar pain
| [34] | Bilterys T, Kregel J, Nijs J, Meeus M, Danneels L, Cagnie B, Van Looveren E, Malfliet A. Influence of education level on the effectiveness of pain neuroscience education: A secondary analysis of a randomized controlled trial. Musculoskelet Sci Pract. 2022; 57: 102494. https://doi.org/10.1016/j.msksp.2021.102494 |
| [35] | Geneen, L. J., Martin, D. J., Adams, N. et al. Effects of education to facilitate knowledge about chronic pain for adults: a systematic review with meta-analysis. Syst Rev. 2015; 132(4): 132. https://doi.org/10.1186/s13643-015-0120-5 |
[34-35]
.
These conflicting findings underscore the complexity of the relationship between education and vulvar dermatosis, suggesting that additional research is needed to better understand the underlying mechanisms and potential contributing factors. It's also essential to consider that women with lower levels of education may be less inclined to seek medical care
| [32] | Bond JC, Harlow BL, White KO. Care Seeking for Chronic Vulvar Pain Among a Large, Population-Based Sample of Reproductive-Aged Women. J Womens Health (Larchmt). 2022 Apr; 31(4): 513-520. https://doi.org/10.1089/jwh.2021.0086 |
[32]
.
Overall, the study's findings provide valuable insights into the demographic and reproductive profiles of patients with vulvar dermatosis. However, it is vital to acknowledge the study's limitations, such as the exclusion of younger patients and the potential impact on the generalizability of the results. Future studies with more extensive and diverse samples, including pediatric populations, would help provide a more comprehensive understanding of vulvar dermatosis across different age groups and improve our knowledge of the condition's underlying causes or risk factors.
5. Conclusion
The DATRIV study provides valuable insights into the demographic and reproductive characteristics of patients with vulvar dermatosis, a form of chronic vulvar discomfort. Key findings include the following:
1) Patients with vulvar dermatosis tend to be older, with a peak incidence in the 45-65 years age range.
2) There is a significant difference in the proportion of patients of reproductive age between the vulvar dermatosis group and other groups, indicating a potential association between hormonal changes and vulvar dermatosis.
3) Patients with vulvar dermatosis have higher weight and BMI than other groups. Patients with vulvar dermatosis are more likely to be married, have a higher number of births, and a higher number of abortions.
4) The vulvar dermatosis group has lower educational levels than other groups.
However, it is essential to acknowledge the study's limitations, including the exclusion of younger patients and potential challenges in generalizing the findings. Future research should aim to include a broader age range, including pediatric populations, to gain a more comprehensive understanding of vulvar dermatosis across different age groups.
In conclusion, the findings of the DATRIV study contribute to our knowledge of the demographic and reproductive characteristics associated with vulvar dermatosis. These findings underscore the importance of considering age, reproductive factors, weight/BMI, and educational status when evaluating and managing patients with vulvar dermatosis. Further research is needed to elucidate the underlying mechanisms and potential causal relationships between these factors and the development of vulvar dermatosis, ultimately leading to improved diagnosis, treatment, and support for affected individuals.
Abbreviations
DATRIV: Diagnostic Accuracy of Three Rings Vulvoscopy
BMI: Body Mass Index
LS: Lichen Sclerosus
TRIV: Three Rings Vulvoscopy
ISSVD: The International Society for the Study of Vulvovaginal Diseases
HRT: hormone replacement therapy
Author Contributions
Vesna Harni: Conceptualization, Resources, Data curation, Formal Analysis, Funding acquisition, Validation, Investigation, Writing - original draft, Methodology, Visualization, Project administration, Writing - review & editing
Damir Babic: Conceptualization, Supervision, Validation, Methodology
Suzana Ljubojevic Hadzavdic: Conceptualization, Formal Analysis, Supervision, Funding acquisition, Validation, Methodology
Dubravko Barisic: Conceptualization, Supervision, Methodology
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
International Association for the Study of Pain, Subcommittee on Taxonomy. Classification of chronic pain. Descriptions of chronic pain syndromes and definitions of pain terms. Pain Supplement 1986; 3: S1-S226.
https://doi.org/10.1097/j.pain.0000000000001939
|
| [2] |
Moyal-Barracco M, Lynch P. 2003 ISSVD terminology and classification vulvodynia: a historical perspective. J Reprod Med 2004; 49: 772-7.
|
| [3] |
Stockdale CK, Lawson HW. 2013 Vulvodynia Guideline update. J Low Genit Tract Dis 2014; 18: 93–100.
https://doi.org/10.1097/LGT.0000000000000021
|
| [4] |
Harlow, BL, Kunitz, CG, Nguyen, RH, Rydell, SA, Turner, RM, MacLehose, RF. Prevalence of symptoms consistent with a diagnosis of vulvodynia: population-based estimates from 2 geographic regions. Am J Obstet Gynecol 2014; 210: 40 e1–8.
https://doi.org/10.1016/j.ajog.2013.09.033
|
| [5] |
Reed, BD, Harlow, SD, Sen, A, Legocki, LJ, Edwards, RM, Arato, N, et al. Prevalence and demographic characteristics of vulvodynia in a population-based sample. Am J Obstet Gynecol 2012; 206: 170 e1–9.
https://doi.org/10.1016/j.ajog.2011.08.012
|
| [6] |
Vieira-Baptista, P, Lima-Silva, J, Cavaco-Gomes, J, Beires, J. Prevalence of vulvodynia and risk factors for the condition in Portugal. Int J Gynaecol Obstet 2014; 127: 283–7.
https://doi.org/10.1016/j.ijgo.2014.05.020
|
| [7] |
Gomez, I, Coronado, PJ, Martin, CM, Alonso, R, Guisasola-Campa, FJ. Study on the prevalence and factors associated to vulvodynia in Spain. Eur J Obstet Gynecol Reprod Biol 2019; 240: 121–4.
https://doi.org/10.1016/j.ejogrb.2019.06.005
|
| [8] |
Edgardh, K, Abdelnoor, M. Longstanding vulval problems and entry dyspareunia among STD-clinic visitors in Oslo-results from a cross-sectional study. Int J STD AIDS 2003; 14: 796–9.
https://doi.org/10.1258/095646203322556101
|
| [9] |
Teigen, Per Kristen, Hagemann, Cecilie Therese, Fors, Egil Andreas, Stauri, Elisabeth, Hoffmann, Risa Lonnée and Schei, Berit. "Chronic vulvar pain in gynecological outpatients" Scandinavian Journal of Pain, 2023; 23 (1): 97-103.
https://doi.org/10.1515/sjpain-2021-0223
|
| [10] |
Loevinger BL, Muller D, Alonso C, Coe CL. Metabolic syndrome in women with chronic pain. Metabolism. 2007; 56(1): 87–93.
https://doi.org/10.1016/j.metabol.2006.09.001
|
| [11] |
Mork PJ, Holtermann A, Nilsen TI. Physical exercise, body mass index and risk of chronic arm pain: longitudinal data on an adult population in Norway. Eur J Pain. 2013; 17(8): 1252–1258.
https://doi.org/10.1002/j.1532-2149.2013.00298.x
|
| [12] |
Hoftun GB, Romundstad PR, Rygg M. Factors associated with adolescent chronic nonspecific pain, chronic multisite pain, and chronic pain with high disability: the Young-HUNT Study 2008. J Pain. 2012; 13(9): 874–883.
https://doi.org/10.1016/j.jpain.2012.06.001
|
| [13] |
Yoo JJ, Cho NH, Lim SH, Kim HA. Relationships between body mass index, fat mass, muscle mass, and musculoskeletal pain in community residents. Arthritis Rheumatol. 2014; 66(12): 3511–3520.
https://doi.org/10.1002/art.38861
|
| [14] |
Groysman V. Vulvodynia: new concepts and review of the literature. Dermatol Clin. 2010; 28: 681-696.
https://doi.org/10.1016/j.det.2010.07.002
|
| [15] |
Falsetta ML, Foster DC, Bonham AD, Phipps RP. A review of the available clinical therapies for vulvodynia management and new data implicating proinflammatory mediators in pain elicitation. BJOG. 2017; 124: 210-218.
https://doi.org/10.1111/1471-0528.14157
|
| [16] |
Thomtén J, Lundahl R, Stigenberg K, Linton S. Fear avoidance and pain catastrophizing among women with sexual pain. Women’s Health (Lond). 2014; 10: 571-581.
https://doi.org/10.2217/whe.14.51
|
| [17] |
Vasileva P, Strashilov SA, Yordanov AD. Aetiology, diagnosis, and clinical management of vulvodynia. Prz Menopauzalny. 2020 Mar; 19(1): 44-48. Epub 2020 Apr 27. PMID: 32699543; PMCID: PMC7258372.
https://doi.org/10.5114/pm.2020.95337
|
| [18] |
Cooper SM, Baldo AM, Wojnarowska F. The association of lichen sclerosus and erosive lichen planus of the vulva with autoimmune disease: a case-control study. Arch Dermatol, 144 (11) (2008), pp. 1432-1435.
https://doi.org/10.1001/archderm.144.11.1432
|
| [19] |
Fistarol SK, Itin PH. Diagnosis and treatment of lichen sclerosus: an update. Am J Clin Dermatol, 14 (1) (2013), pp. 27-47.
https://doi.org/10.1007/s40257-012-0006-4
|
| [20] |
Schlosser BJ, Mirowski GW. Lichen sclerosus and lichen planus in women and girls. Clin Obstet Gynecol, 58 (1) (2015), pp. 125-142.
https://doi.org/10.1097/GRF.0000000000000090
|
| [21] |
Melnick LE, Steuer AB, Bieber AK, Wong PW, Pomeranz MK. Lichen sclerosus among women in the United States. Int J Womens Dermatol. 2020 May 8; 6(4): 260-262. PMID: 33015282; PMCID: PMC7522895.
https://doi.org/10.1016/j.ijwd.2020.05.001
|
| [22] |
Trokoudes D, Lewis FM. Lichen sclerosus - the course during pregnancy and effect on delivery. J Eur Acad Dermatol Venereol, 33 (12) (2019), pp. e466-e468.
https://doi.org/10.1111/jdv.15788
|
| [23] |
M. Yang, W. Wen, J. Chang J. Vulvar lichen sclerosus: a single-center retrospective study in China. J Dermatol, 45 (9) (2018), pp. 1101-1104.
https://doi.org/10.1111/1346-8138.14533
|
| [24] |
Powell, A. M., Sarria, I. & Goje, O. Role of Obesity in Recurrent Vulvovaginal Symptoms and Disease. Curr Infect Dis Rep 25, 1–6 (2023).
https://doi.org/10.1007/s11908-022-00793-2
|
| [25] |
Tan IF, AW. Chapter 31 - Obesity and chronic pelvic pain, Editor(s): Tahir A. Mahmood, Sabaratnam Arulkumaran, Frank A. Chervenak, Obesity and Gynecology (Second Edition), Elsevier, 2020: 281-291, ISBN 9780128179192,
https://doi.org/10.1016/B978-0-12-817919-2.00031-0
|
| [26] |
Okifuji A, Hare BD. The association between chronic pain and obesity. J Pain Res. 2015 Jul 14; 8: 399-408. PMID: 26203274; PMCID: PMC4508090.
https://doi.org/10.2147/JPR.S55598
|
| [27] |
Pudalov LR, Krause SJ, Heinberg LJ, Hogue O. Refractory Chronic Pain and Obesity: Promising Implications for Multidisciplinary Pain Rehabilitation, Pain Medicine, 2021; 22 (10): 2290–2297,
https://doi.org/10.1093/pm/pnab055
|
| [28] |
Bachmann GA, Rosen R, Arnold LD, Burd I, Rhoads GG, Leiblum SR, Avis N. Chronic vulvar and other gynecologic pain: prevalence and characteristics in a self-reported survey. J Reprod Med. 2006 Jan; 51(1): 3-9.
|
| [29] |
Reed BD, Crawford S, Couper M, et al. Pain at the Vulvar Vestibule: A Web-Based Survey. J Low Genit Tract Dis 2004; 8: 48-57.
https://doi.org/10.1097/00128360-200401000-00011
|
| [30] |
Sadownik LA. Clinical profile of vulvodynia patients. A prospective study of 300 patients. J Reprod Med. 2000 Aug; 45(8): 679-84.
|
| [31] |
Shaik H, Konala S, Kolalapudi SA, Alluri R, Godha V, Navya B. Clinical and Demographic Patterns of Vulval Dermatoses and Their Impact on Quality of Life. Indian Dermatol Online J. 2022 Dec 14; 14(1): 44-49.
https://doi.org/10.4103/idoj.idoj_339_22
|
| [32] |
Bond JC, Harlow BL, White KO. Care Seeking for Chronic Vulvar Pain Among a Large, Population-Based Sample of Reproductive-Aged Women. J Womens Health (Larchmt). 2022 Apr; 31(4): 513-520.
https://doi.org/10.1089/jwh.2021.0086
|
| [33] |
Joypaul S, Kelly F, McMillan SS, King MA. Multi-disciplinary interventions for chronic pain involving education: A systematic review. PLOS. 2019,
https://doi.org/10.1371/journal.pone.0223306
|
| [34] |
Bilterys T, Kregel J, Nijs J, Meeus M, Danneels L, Cagnie B, Van Looveren E, Malfliet A. Influence of education level on the effectiveness of pain neuroscience education: A secondary analysis of a randomized controlled trial. Musculoskelet Sci Pract. 2022; 57: 102494.
https://doi.org/10.1016/j.msksp.2021.102494
|
| [35] |
Geneen, L. J., Martin, D. J., Adams, N. et al. Effects of education to facilitate knowledge about chronic pain for adults: a systematic review with meta-analysis. Syst Rev. 2015; 132(4): 132.
https://doi.org/10.1186/s13643-015-0120-5
|
| [36] |
Harni V, Babic D, Hadzavdic S, Barisic D. Diagnostic Accuracy of the Vulvoscopy Index for Detection of Vulvar Dermatosis (DATRIV Study, Part 1). Journal of Gynecology and Obstetrics 2022; Vol. 10, No. 1, 39-47.
https://doi.org/10.11648.j.jgo.20221001.16
|
| [37] |
Harni V, Babic D, Hadzavdic S, Barisic D. Clinical Value of the N-S-P Scheme for Detection of Vulvar Dermatosis (DATRIV Study, Part 2). Journal of Gynecology and Obstetrics 2022; Vol. 10, No. 3, 159-166.
https://doi.org/10.11648.j.jgo.20221003.11
|
| [38] |
Bornstein J, Sideri M, Tatti S, Walker P, Prendiwille W, Haefner HK. 2011 Terminology of the Vulva of the International Federation for Cervical Pathology and Colposcopy. J Lower Genit Tract Dis 2012; 16: 290-5.
https://doi.org/10.1097/LGT.0b013e31825934c7
|
| [39] |
van Beurden M, van der Vange N, de Craen AJM, Tjong-A-Hung SP, ten Kate FJW, ter Schegget J, et al. Normal findings in vulvar examination and vulvoscopy. J Br Obstet Gynaecol 1997; 104: 320-4.
https://doi.org/10.1111/j.1471-0528.1997.tb11461.x
|
| [40] |
Byrne MA, Walker MM, Leonard J, Pryce D, Taylor-Robinson D. Recognising covert disease in women with chronic vulval symptoms attending an STD clinic: value of detailed examination including colposcopy. Genitourin Med 1989; 65: 46-9.
https://doi.org/10.1136/sti.65.1.46
|
| [41] |
Audisio T, Zarazaga J, Vainer O. A Classification of Vulvoscopic Findings for Clinical Diagnosis. J Lower Genit Tract Dis 1999; 3: 7-18.
https://doi.org/10.1046/j.1526-0976.1999.08079.x.
|
| [42] |
Harni V, Babic D, Barisic D. "Three Rings Vulvoscopy" – A New Approach to the Vulva. Gynaecol Perinatol 2015; 24: 37-45.
|
| [43] |
Harni V, Babic D, Barisic D. "Three Rings Vulvoscopy" – A New Approach to the Vulva. Chapter in Watson L (ed.) Cryosurgery and Colposcopy: Practices, Outcomes, and Potential Complications. New York, Nova Science Publishers Inc; 2016. ISBN: 978-1-63484-507-6.
|
| [44] |
Friedrich EG Jr. Vulvar vestibulitis syndrome. J Reprod Med 1987; 32: 110-4.
|
| [45] |
Haefner H, Collins M, Davis GD, Edwards L, Foster D, Hartmann E, et al. The Vulvodynia Guideline. J Lower Genit Tract Dis 2005; 9: 40-51.
https://doi.org/10.1097/00128360-200501000-00009
|
| [46] |
Jantos M, Burns NR. Vulvodynia. Development of a psychosexual profile. J Reprod Med. 2007 Jan; 52(1): 63-71.
|
| [47] |
Patla G, Mazur-Bialy AI, Humaj-Grysztar M, Bonior J. Chronic Vulvar Pain and Health-Related Quality of Life in Women with Vulvodynia. Life (Basel). 2023 Jan 24; 13(2): 328.
https://doi.org/10.3390/life13020328
|
| [48] |
Driul L, Bertozzi S, Londero AP, Fruscalzo A, Rusalen A, Marchesoni D, Di Benedetto P. Risk factors for chronic pelvic pain in a cohort of primipara and secondipara at one year after delivery: association of chronic pelvic pain with autoimmune pathologies. Minerva Ginecol. 2011 Apr; 63(2): 181-7.
|
Cite This Article
-
APA Style
Harni, V., Babic, D., Hadzavdic, S. L., Barisic, D. (2024). Basic Characteristics and Demographic Data in Patients with Chronic Vulvar Discomfort: A Detailed Analysis of DATRIV Study. Journal of Gynecology and Obstetrics, 12(2), 35-45. https://doi.org/10.11648/j.jgo.20241202.14
 Copy
|
Copy
|
 Download
Download
ACS Style
Harni, V.; Babic, D.; Hadzavdic, S. L.; Barisic, D. Basic Characteristics and Demographic Data in Patients with Chronic Vulvar Discomfort: A Detailed Analysis of DATRIV Study. J. Gynecol. Obstet. 2024, 12(2), 35-45. doi: 10.11648/j.jgo.20241202.14
Copy
|
Download
AMA Style
Harni V, Babic D, Hadzavdic SL, Barisic D. Basic Characteristics and Demographic Data in Patients with Chronic Vulvar Discomfort: A Detailed Analysis of DATRIV Study. J Gynecol Obstet. 2024;12(2):35-45. doi: 10.11648/j.jgo.20241202.14
Copy
|
Download
-
@article{10.11648/j.jgo.20241202.14,
author = {Vesna Harni and Damir Babic and Suzana Ljubojevic Hadzavdic and Dubravko Barisic},
title = {Basic Characteristics and Demographic Data in Patients with Chronic Vulvar Discomfort: A Detailed Analysis of DATRIV Study
},
journal = {Journal of Gynecology and Obstetrics},
volume = {12},
number = {2},
pages = {35-45},
doi = {10.11648/j.jgo.20241202.14},
url = {https://doi.org/10.11648/j.jgo.20241202.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.jgo.20241202.14},
abstract = {This study aims to provide a descriptive analysis of the essential characteristics and demographic profiles, including age, weight, height, body mass index, marital status, and educational background in patients with chronic vulvar discomfort. The data were collected from the study DATRIV (Diagnostic Accuracy of Three Rings Vulvoscopy), which included 328 participants divided into four groups: normal vulva, impaired vulvar skin, primary vulvar distress/vulvodynia, and secondary discomfort caused by vulvar dermatoses. The clinical data collected from the study questionnaire were analyzed using statistical software such as StatSoft (Dell, Austin, TX, USA), Statistica 12 (TIBCO®, Palo Alto, CA, USA), and SPSS 20 (IBM, Armonk, NY, USA). The study was conducted with the approval of the Institutional Review Board of Polyclinic Harni, and all participants provided written informed consent. The findings from the DATRIV study shed light on several important aspects of chronic vulvar discomfort. They offered valuable insights into the demographic and reproductive characteristics of patients with chronic vulvar pain, specifically vulvar dermatosis. The study revealed that patients with vulvar dermatosis tended to be older, with a peak incidence in the 45-65 age range. They also had higher weight and BMI compared to other groups. There was a significant difference in the proportion of patients of reproductive age between the vulvar dermatosis group and other groups. Additionally, the vulvar dermatosis group had higher rates of marriage, births, and abortions and lower educational levels. The study's limitations included lacking patients younger than 16 years. Future research should aim to include a broader age range, including pediatric populations, to gain a more comprehensive understanding of vulvar dermatosis across different age groups. Further investigation is needed to uncover the underlying mechanisms and establish causal relationships, enhancing diagnosis, treatment, and support for individuals affected by vulvar dermatosis.
},
year = {2024}
}
Copy
|
Download
-
TY - JOUR
T1 - Basic Characteristics and Demographic Data in Patients with Chronic Vulvar Discomfort: A Detailed Analysis of DATRIV Study
AU - Vesna Harni
AU - Damir Babic
AU - Suzana Ljubojevic Hadzavdic
AU - Dubravko Barisic
Y1 - 2024/04/28
PY - 2024
N1 - https://doi.org/10.11648/j.jgo.20241202.14
DO - 10.11648/j.jgo.20241202.14
T2 - Journal of Gynecology and Obstetrics
JF - Journal of Gynecology and Obstetrics
JO - Journal of Gynecology and Obstetrics
SP - 35
EP - 45
PB - Science Publishing Group
SN - 2376-7820
UR - https://doi.org/10.11648/j.jgo.20241202.14
AB - This study aims to provide a descriptive analysis of the essential characteristics and demographic profiles, including age, weight, height, body mass index, marital status, and educational background in patients with chronic vulvar discomfort. The data were collected from the study DATRIV (Diagnostic Accuracy of Three Rings Vulvoscopy), which included 328 participants divided into four groups: normal vulva, impaired vulvar skin, primary vulvar distress/vulvodynia, and secondary discomfort caused by vulvar dermatoses. The clinical data collected from the study questionnaire were analyzed using statistical software such as StatSoft (Dell, Austin, TX, USA), Statistica 12 (TIBCO®, Palo Alto, CA, USA), and SPSS 20 (IBM, Armonk, NY, USA). The study was conducted with the approval of the Institutional Review Board of Polyclinic Harni, and all participants provided written informed consent. The findings from the DATRIV study shed light on several important aspects of chronic vulvar discomfort. They offered valuable insights into the demographic and reproductive characteristics of patients with chronic vulvar pain, specifically vulvar dermatosis. The study revealed that patients with vulvar dermatosis tended to be older, with a peak incidence in the 45-65 age range. They also had higher weight and BMI compared to other groups. There was a significant difference in the proportion of patients of reproductive age between the vulvar dermatosis group and other groups. Additionally, the vulvar dermatosis group had higher rates of marriage, births, and abortions and lower educational levels. The study's limitations included lacking patients younger than 16 years. Future research should aim to include a broader age range, including pediatric populations, to gain a more comprehensive understanding of vulvar dermatosis across different age groups. Further investigation is needed to uncover the underlying mechanisms and establish causal relationships, enhancing diagnosis, treatment, and support for individuals affected by vulvar dermatosis.
VL - 12
IS - 2
ER -
Copy
|
Download