Abstract
Acute-on-chronic liver failure (ACLF) is a distinct clinical syndrome characterized by acute hepatic deterioration in patients with underlying chronic liver disease and is associated with multiorgan dysfunction and high short-term mortality. In India, alcohol remains the predominant etiology of chronic liver disease, with infectious causes and alcoholic hepatitis being common acute precipitating events. However, clinical profiles and predictors of in-hospital outcomes show variability across populations. This hospital-based observational study included 50 patients diagnosed with ACLF according to the APASL criteria and admitted to Aakash Healthcare Super Speciality Hospital, New Delhi, between February 2024 and January 2026. Detailed clinical evaluation and laboratory investigations were performed at admission. Disease severity was assessed using Child–Turcotte–Pugh, Model for End-Stage Liver Disease (MELD), and MELD-Na scores. Precipitating factors, complications, organ system involvement, and outcomes during hospitalization were documented. Outcomes were categorized as survival with discharge, in-hospital mortality, or referral for liver transplantation. The mean age of patients was 49.96 ± 11.30 years, with a male predominance (84%). Alcohol-related liver disease was the most common underlying etiology (60%). Alcoholic hepatitis (38%) and sepsis (30%) were the leading precipitating events. Jaundice, abdominal distension, and altered sensorium were the most frequent presenting symptoms. Ascites (96%), portal hypertension (92%), and hepatic encephalopathy (78%) were the predominant complications. In-hospital mortality was observed in 46% of patients, while 22% required referral for liver transplantation. Elevated international normalized ratio, serum creatinine, ammonia, lactate, serum potassium levels, and higher MELD and MELD-Na scores were significantly associated with poor outcomes (p < 0.05). Hepatic encephalopathy was the only clinical complication significantly associated with mortality on univariate analysis (p = 0.021). ACLF predominantly affects middle-aged males with alcohol-related chronic liver disease and is associated with high in-hospital mortality. Early identification of high-risk patients and timely escalation of care, including prompt evaluation for liver transplantation, are crucial to improving outcomes.
|
Published in
|
International Journal of Gastroenterology (Volume 10, Issue 1)
|
|
DOI
|
10.11648/j.ijg.20261001.13
|
|
Page(s)
|
9-19 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2026. Published by Science Publishing Group
|
Keywords
Acute-on-chronic Liver Failure, Alcoholic Hepatitis, Chronic Liver Disease, Hepatic Encephalopathy, MELD-Na Score, Liver Transplantation
1. Introduction
1.1. Definition and Overview of Acute-on-chronic Liver Failure
Acute-on-chronic liver failure (ACLF) is a distinct clinical syndrome characterized by acute deterioration of liver function in patients with pre-existing chronic liver disease (CLD), frequently accompanied by multiorgan dysfunction and high short-term mortality
. Unlike simple acute decompensation of cirrhosis, ACLF represents a unique clinical entity driven by intense systemic inflammation, rapid progression, and a potentially reversible course if recognized and managed early. Contemporary global analyses have further reinforced ACLF as a heterogeneous syndrome with variable clinical phenotypes and outcomes depending on the number and type of organ failures
| [2] | Aggarwal, A., Biswas, S., Arora, U., Vaishnav, M., Shenoy, A., Swaroop, S., Agarwal, A., Elhence, A., Kumar, R., Goel, A., & Shalimar (2024). Definitions, Etiologies, and Outcomes of Acute on Chronic Liver Failure: A Systematic Review and Meta-analysis. Clinical gastroenterology and hepatology: the official clinical practice journal of the American Gastroenterological Association, 22(11), 2199–2210. e25.
https://doi.org/10.1016/j.cgh.2024.04.018 |
[2]
.
1.2. Comparison of Definitions: APASL, EASL–AASLD, and WGO
Multiple international liver societies have proposed definitions for ACLF, reflecting differences in patient populations and clinical perspectives.
The definition proposed by the Asian Pacific Association for the Study of the Liver (APASL) emphasizes an acute hepatic insult in patients with previously diagnosed or undiagnosed CLD. It is characterized by jaundice (serum bilirubin ≥5 mg/dL) and coagulopathy (international normalized ratio ≥1.5), complicated within four weeks by ascites and/or hepatic encephalopathy
| [3] | Sarin SK, Kumar A, Almeida JA, Chawla YK, Fan ST, Garg H, et al. Acute-on-chronic liver failure: consensus recommendations of the Asian Pacific Association for the Study of the Liver. Hepatology International. 2009; 3(1): 269–282.
https://doi.org/10.1007/s12072-008-9106-x |
[3]
.
In contrast, the definition by the European Association for the Study of the Liver and the American Association for the Study of Liver Diseases focuses on acute decompensation of cirrhosis due to hepatic or extrahepatic insults, leading to organ failure and high 28- to 90-day mortality
| [4] | Moreau R, Jalan R, Gines P, Pavesi M, Angeli P, Cordoba J, et al. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology. 2013; 144(7): 1426–1437.
https://doi.org/10.1053/j.gastro.2013.02.042 |
[4]
.
To harmonize these perspectives, the World Gastroenterology Organisation proposed a unified framework that incorporates both concepts and stratifies patients based on the severity of underlying liver disease into non-cirrhotic CLD, compensated cirrhosis, and decompensated cirrhosis
| [5] | Jalan R, Yurdaydin C, Bajaj JS, Acharya SK, Arroyo V, Lin H-C, et al. Toward an improved definition of acute-on-chronic liver failure. Gastroenterology. 2014; 147(1): 4–10.
https://doi.org/10.1053/j.gastro.2014.05.005 |
[5]
.
1.3. Pathophysiology and Disease Progression
The pathogenesis of ACLF is best explained by a “two-hit” model. The first hit is the presence of underlying CLD, commonly due to chronic alcohol use, viral hepatitis, or metabolic dysfunction–associated steatotic liver disease. The second hit is an acute precipitating event such as infection, alcoholic hepatitis, gastrointestinal bleeding, or drug-induced liver injury. This triggers an exaggerated systemic inflammatory response with cytokine release, immune dysregulation, and circulatory dysfunction, culminating in multiorgan failure
| [6] | Sarin SK, Choudhury A. Acute-on-chronic liver failure: terminology, mechanisms and management. Nature Reviews Gastroenterology & Hepatology. 2016; 13: 131–149.
https://doi.org/10.1038/nrgastro.2015.219 |
| [7] | Verbeke L, Nevens F, Laleman W. Bench-to-bedside review: acute-on-chronic liver failure—linking the gut, liver and systemic circulation. Critical Care. 2011; 15: 233.
https://doi.org/10.1186/cc10424 |
[6, 7]
. As a result, there is rapid deterioration in hepatic synthetic function along with extrahepatic organ involvement, particularly affecting the kidneys, brain, and cardiovascular system.
1.4. Clinical Significance and Prognostic Assessment
ACLF is associated with extremely high short-term mortality, with reported 28-day mortality rates approaching 40–50% among hospitalized patients
| [8] | Shalimar, Saraswat V, Singh SP, Duseja A, Shukla A, Eapen CE, et al. Acute-on-chronic liver failure in India: the Indian National Association for Study of the Liver consortium experience. Journal of Gastroenterology and Hepatology. 2016; 31(10): 1742–1749. https://doi.org/10.1111/jgh.13313 |
[8]
. Unlike stable decompensated cirrhosis, ACLF requires intensive monitoring, early organ support, and prompt risk stratification to identify patients who may benefit from urgent liver transplantation. Prognostic scoring systems such as the Model for End-Stage Liver Disease (MELD) and MELD-Na scores are widely used in clinical practice to assess disease severity and predict short-term outcomes in patients with ACLF
| [9] | Zhang Q, Guo X, Zhao S, Pang X, Wang Y, Zhang Y, Chi B. Prognostic performance of clinical indices and model scorings for acute-on-chronic liver failure: a study of 164 patients. Experimental and Therapeutic Medicine. 2016; 11(4): 1348–1354. https://doi.org/10.3892/etm.2016.3037 |
[9]
.
Recent large cohort studies have further evaluated early predictors of organ failure progression and mortality, highlighting the importance of dynamic risk assessment models in improving clinical decision-making
| [10] | Shen, Y., Xu, W., Chen, Y. et al. Early prediction of acute-on-chronic liver failure development in patients with diverse chronic liver diseases. Sci Rep 14, 28245 (2024).
https://doi.org/10.1038/s41598-024-79486-w |
[10]
.
In addition to conventional supportive management and consideration for liver transplantation, recent therapeutic advances have explored extracorporeal liver support systems aimed at modulating systemic inflammation and improving organ function. A randomized controlled trial evaluating the DIALIVE liver dialysis device demonstrated safety and potential clinical benefits in patients with acute-on-chronic liver failure, highlighting the evolving landscape of adjunctive therapies in this high-risk population
| [11] | Agarwal, B., Cañizares, R. B., Saliba, F., Ballester, M. P., Tomescu, D. R., Martin, D., Stadlbauer, V., Wright, G., Sheikh, M., Morgan, C., Alzola, C., Lavin, P., Green, D., Kumar, R., Sacleux, S. C., Schilcher, G., Koball, S., Tudor, A., Minten, J., Domenech, G., … Jalan, R. (2023). Randomized, controlled clinical trial of the DIALIVE liver dialysis device versus standard of care in patients with acute-on- chronic liver failure. Journal of hepatology, 79(1), 79–92.
https://doi.org/10.1016/j.jhep.2023.03.013 |
[11]
.
1.5. Regional Epidemiology and Disease Burden
The epidemiology of ACLF varies significantly across geographic regions due to differences in the etiologies of underlying CLD. In India and other South Asian countries, alcohol-related liver disease is the leading cause of CLD and a major precipitating factor for ACLF
| [8] | Shalimar, Saraswat V, Singh SP, Duseja A, Shukla A, Eapen CE, et al. Acute-on-chronic liver failure in India: the Indian National Association for Study of the Liver consortium experience. Journal of Gastroenterology and Hepatology. 2016; 31(10): 1742–1749. https://doi.org/10.1111/jgh.13313 |
[8]
. In Western populations, metabolic dysfunction–associated steatotic liver disease is increasingly prevalent, while alcohol-related injury and sepsis remain common triggers for ACLF
| [5] | Jalan R, Yurdaydin C, Bajaj JS, Acharya SK, Arroyo V, Lin H-C, et al. Toward an improved definition of acute-on-chronic liver failure. Gastroenterology. 2014; 147(1): 4–10.
https://doi.org/10.1053/j.gastro.2014.05.005 |
[5]
.
Reviews from Western populations have highlighted differences in the epidemiology, precipitating factors, and clinical outcomes of acute-on-chronic liver failure when compared with Asian cohorts, underscoring the heterogeneity of the syndrome across geographic regions
.
In North American cohorts, acute-on-chronic liver failure has been predominantly described in the setting of infection-related decompensation and organ failure, as defined by the North American Consortium for the Study of End-Stage Liver Disease (NACSELD) criteria, which emphasize short-term mortality and extrahepatic organ dysfunction
| [13] | Bajaj JS, et al. Acute-on-chronic liver failure defined by North American Consortium for the Study of End-Stage Liver Disease criteria. Hepatology. 2014; 60(6): 1853–1861.
https://doi.org/10.1002/hep.27323 |
[13]
. Recent multinational cohort analyses have further confirmed significant geographic variability in precipitating events, organ failure patterns, and survival outcomes, reinforcing ACLF as a clinically heterogeneous syndrome across diverse global populations
. These regional differences influence clinical presentation, disease progression, and outcomes.
1.6. Rationale for the Present Study
Despite increasing recognition of ACLF as a distinct clinical entity, hospital outcomes vary widely due to differences in precipitating events, healthcare infrastructure, and timing of intervention. Limited data are available from tertiary care centers in North India regarding the clinical profile of ACLF and the factors influencing in-hospital outcomes. Understanding the association between clinical characteristics at admission and short-term outcomes such as survival, mortality, or referral for liver transplantation is essential for early risk stratification and optimized patient management. Therefore, the present study aims to evaluate the clinical profile of patients with ACLF and identify predictors of hospital outcomes in a tertiary care setting.
2. Materials and Methods
2.1. Study Area and Setting
This study was conducted at Aakash Healthcare Super Speciality Hospital, located at Road No. 201, Sector-3, Dwarka, New Delhi-110075. Patients were enrolled from the Departments of Medicine and Gastroenterology & Hepatology.
2.2. Study Design and Duration
This was a prospective observational study carried out over a period of two years, from February 2024 to January 2026.
2.3. Ethical Considerations
The study was conducted in accordance with the ethical principles of the Declaration of Helsinki. Ethical approval was obtained from the Institutional Ethics Committee of Aakash Healthcare Super Speciality Hospital, Delhi, India (Approval No.: AHPL/Academis/DNB-2023/2024). Written informed consent was obtained from all participants or their legally authorized representatives prior to enrollment. Confidentiality and anonymity of patient data were strictly maintained throughout the study.
2.4. Study Population
The study included patients admitted with a diagnosis of acute-on-chronic liver failure during the study period.
2.4.1. Inclusion Criteria
Patients with acute hepatic insults, with or without prior hepatic decompensation, who were diagnosed with ACLF according to the Asian Pacific Association for the Study of the Liver (APASL) definition were included in the study.
2.4.2. Exclusion Criteria
Patients with hepatocellular carcinoma and those who refused or were unable to provide informed consent were excluded from the study.
2.4.3. Diagnostic Criteria
ACLF was diagnosed according to the APASL definition as acute hepatic insult manifesting as jaundice (serum bilirubin >5 mg/dL) and coagulopathy (international normalized ratio >1.5), complicated within four weeks by ascites and/or hepatic encephalopathy in patients with previously diagnosed or undiagnosed chronic liver disease
| [3] | Sarin SK, Kumar A, Almeida JA, Chawla YK, Fan ST, Garg H, et al. Acute-on-chronic liver failure: consensus recommendations of the Asian Pacific Association for the Study of the Liver. Hepatology International. 2009; 3(1): 269–282.
https://doi.org/10.1007/s12072-008-9106-x |
[3]
.
The diagnosis of cirrhosis was established based on clinical features, biochemical parameters, radiological findings, or prior liver biopsy records.
Acute hepatic insults included viral superinfection (hepatitis A virus or hepatitis E virus), viral reactivation (hepatitis B virus), ongoing alcohol consumption, autoimmune flare, and drug-induced liver injury (anti-tuberculosis drugs or antiepileptics). Non-hepatic precipitating events included variceal bleeding and sepsis, such as spontaneous bacterial peritonitis, urinary tract infection, respiratory tract infection, cellulitis, and spontaneous bacteremia.
Silent chronic liver disease was defined as previously undiagnosed CLD without any prior episode of decompensation, whereas overt CLD referred to patients with a known diagnosis of cirrhosis, with or without previous decompensation.
2.5. Sample Size
The study aimed to evaluate the relationship between the presenting clinical profile and hospital outcomes in patients with ACLF. Based on available literature, the prevalence of APASL-defined ACLF was estimated to be 14.6%. Using a confidence level of 95% and an absolute precision of 10%, the calculated sample size was 48, which was rounded off to 50 patients.
2.6. Treatment Protocol
All patients received standard medical care as per institutional protocols. No experimental interventions were undertaken.
2.7. Data Collection
Data were collected using a predefined proforma and included demographic variables such as age and gender, detailed clinical history, physical examination findings, laboratory parameters, Child–Turcotte–Pugh score, Model for End-Stage Liver Disease score, and MELD-Na score. The etiology of underlying chronic liver disease and the precipitating cause of ACLF were also documented.
2.8. Outcome Measures
Patients were followed throughout their hospital stay, and outcomes were categorized as survival with discharge, in-hospital mortality, or referral for liver transplantation. These groups were analyzed separately.
2.9. Statistical Analysis
All data were recorded in a predetermined proforma and entered into Microsoft Excel 2016. Statistical analysis was performed using SPSS software version 20. Categorical variables were expressed as frequencies and percentages, while continuous variables were presented as mean ± standard deviation. Comparisons between two groups were performed using Student’s t-test or the Mann–Whitney U test, as appropriate. For multiple group comparisons, analysis of variance (ANOVA) was applied.
Associations between clinical and laboratory parameters and in-hospital mortality were evaluated using univariate analysis. Due to the limited sample size and number of outcome events, multivariate logistic regression analysis was not performed to avoid model overfitting.
A p-value of less than 0.05 was considered statistically significant.
3. Results
3.1. Demographic Characteristics
3.1.1. Age
The mean age of the study population was 49.96 ± 11.30 years. This indicates that most of the patients in the study were in the middle-age group.
Figure 1. Mean age of study population.
3.1.2. Gender Distribution
Male patients constituted the majority of the study population, with 84% males (n = 42) and 16% females (n = 8).
Figure 2. Gender distribution of study population.
3.2. Clinical Profile
3.2.1. Clinical Symptoms
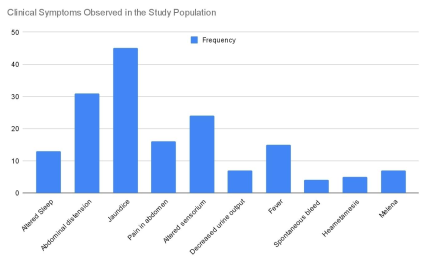
The most common presenting symptom was jaundice (90%), followed by abdominal distension (62%), altered sensorium (48%), and pain in the abdomen (32%). Fever was present in 30% and decreased urine output in 14% of patients. Gastrointestinal bleeding symptoms included hematemesis (10%) and melena (14%).
Figure 3. Clinical symptoms observed in study population.
3.2.2. Clinical Signs
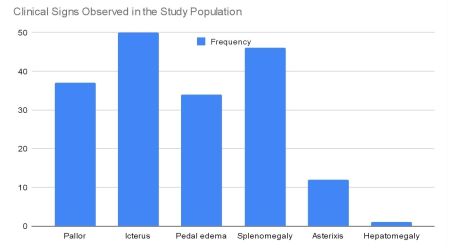
On examination, icterus was observed in all patients (100%). Other common signs included splenomegaly (92%), pedal edema (68%), and pallor (74%). Asterixis was seen in 24% of patients, and hepatomegaly in 2%.
Figure 4. Clinical signs observed in study population.
3.3. Etiology
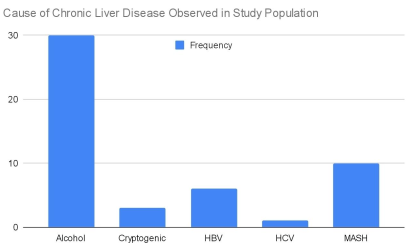
3.3.1. Cause of Chronic Liver Disease
Alcohol was the most common etiology (60%), followed by MASH (20%), HBV (12%), Cryptogenic (6%) and HCV (2%).
Figure 5. Cause of chronic liver disease observed in study population.
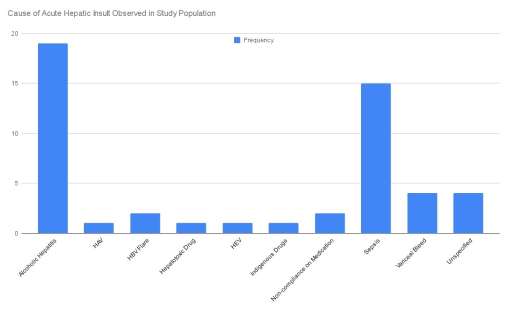
3.3.2. Cause of Acute Hepatic Insult
Alcoholic hepatitis was the leading cause of acute hepatic insult, accounting for 38% of patients. Sepsis was the second most common precipitating factor, observed in 30% of patients. Variceal bleeding was noted in 8% of cases, while no identifiable precipitating cause was found in 8% of patients. Other less frequent causes included hepatitis A virus (HAV) infection, hepatitis B virus (HBV) flare, hepatitis E virus (HEV) infection, hepatotoxic drugs, and indigenous medications.
Figure 6. Cause of acute hepatic insult observed in study population.
3.4. Laboratory Parameters
Significant associations were observed between several laboratory parameters and patient outcomes. Among hematological parameters, hemoglobin (p = 0.037) and international normalized ratio (p < 0.001) showed statistically significant differences between outcome groups, with higher INR values observed among patients with poor outcomes. Prothrombin time demonstrated a trend towards significance (p = 0.051).
Analysis of liver function tests demonstrated that total serum bilirubin (p = 0.033) was significantly associated with outcomes, with higher values observed in patients who experienced in-hospital mortality or required referral for liver transplantation. Other liver enzymes, including alanine aminotransferase and aspartate aminotransferase, were higher in the mortality group but did not show statistically significant associations.
Among serum electrolytes, potassium levels were significantly higher in the mortality group compared with survivors (p = 0.008).
Renal function and metabolic parameters showed strong associations with outcomes. Serum creatinine (p = 0.017), serum ammonia (p = 0.002), and serum lactate levels (p = 0.001) were significantly elevated among non-survivors, indicating a higher burden of organ dysfunction in this group.
Table 1. Comparison of Laboratory Parameters among Different Patient Outcome Groups.
Parameters | Survival with Discharge | In-hospital Mortality | Referral for Liver Transplantation | P - Value |
Hemoglobin | 9.76 | 8.32 | 9.48 | 0.037 |
Total Leukocyte count | 7836.25 | 11999.13 | 8496.36 | 0.135 |
Platelet count | 78531.25 | 93434.78 | 79090.91 | 0.688 |
Prothrombin time | 22.11 | 34.78 | 24.78 | 0.051 |
International Normalized Ratio | 1.90 | 3.65 | 2.18 | <0.001 |
Total Bilirubin | 6.53 | 7.12 | 10.88 | 0.033 |
Alkaline phosphatase | 163.5 | 134.22 | 159.73 | 0.336 |
Alanine Aminotransferase | 103.18 | 441.80 | 74.33 | 0.317 |
Aspartate Aminotransferase | 222.43 | 337.06 | 165.37 | 0.493 |
Serum albumin | 2.54 | 2.57 | 2.76 | 0.532 |
Serum sodium | 135.50 | 132.65 | 133.82 | 0.511 |
Serum potassium | 3.98 | 4.46 | 3.68 | 0.008 |
Serum creatinine | 1.09 | 1.84 | 0.99 | 0.017 |
Serum ammonia | 69.58 | 126.20 | 65.23 | 0.002 |
Serum lactate | 2.59 | 3.99 | 1.38 | 0.001 |
3.5. Complications and Outcomes
Hepatic encephalopathy was significantly associated with adverse patient outcomes (p = 0.021). Other complications, including ascites, portal hypertension, and variceal bleeding, did not show a statistically significant association with outcomes.
Table 2. Association of Complications Observed with Patient Outcome Groups.
Complications | Survival with Discharge | In-hospital Mortality | Referral for Liver Transplantation | P- Value |
Ascites | 15 | 23 | 10 | 0.384 |
Portal Hypertensive Gastropathy | 14 | 21 | 11 | 0.494 |
Hepatic encephalopathy | 10 | 22 | 7 | 0.021 |
Portal Hypertension | 14 | 22 | 10 | 0.646 |
Hepatorenal Syndrome | 2 | 8 | 1 | 0.129 |
Gastroesophageal Variceal Bleeding | 6 | 11 | 3 | 0.504 |
3.6. Liver Disease Severity Scores
All liver disease severity scores showed significant associations with patient outcomes. Child–Turcotte–Pugh score (p = 0.001), Model for End-Stage Liver Disease score (p < 0.001), and MELD-Na score (p < 0.001) were significantly higher in the in-hospital mortality group compared with survivors. Differences were observed across the three outcome groups.
Table 3. Comparison of Liver Disease Severity Score among Different Patient Outcome Groups.
Scores | Survival with Discharge | In-hospital Mortality | Referral for Liver Transplantation | P - Value |
CTP | 11.88 ± 1.15 | 13.39 ± 1.34 | 11.36 ± 2.16 | 0.001 |
MELD | 22.25 ± 2.70 | 31.83 ± 5.46 | 24.91 ± 6.22 | < 0.001 |
MELD-Na | 23.38 ± 2.68 | 33.17 ± 5.07 | 26.27 ± 7.21 | < 0.001 |
4. Discussion
4.1. Overview of Acute-on-chronic Liver Failure
Acute-on-chronic liver failure (ACLF) is a distinct clinical entity characterized by an acute hepatic insult in patients with underlying chronic liver disease, resulting in rapid deterioration of liver function and failure of one or more extrahepatic organs. Several international definitions of ACLF have been proposed, including those by the Asian Pacific Association for the Study of the Liver, the European Association for the Study of the Liver–Chronic Liver Failure Consortium, and the North American Consortium for the Study of End-Stage Liver Disease. Although these definitions differ in diagnostic criteria and emphasis, all underscore the central role of precipitating events, systemic inflammation, and multiorgan dysfunction in determining patient outcomes. Studies by Jalan et al. and Moreau et al. have highlighted ACLF as a heterogeneous syndrome with marked variability in etiology, clinical presentation, and prognosis across different geographic regions
| [1] | Jalan R, Gines P, Olson JC, Mookerjee RP, Moreau R, Garcia-Tsao G, et al. Acute-on-chronic liver failure. Journal of Hepatology. 2012; 57(6): 1336–1348. https://doi.org/10.1016/j.jhep.2012.06.026 |
| [4] | Moreau R, Jalan R, Gines P, Pavesi M, Angeli P, Cordoba J, et al. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology. 2013; 144(7): 1426–1437.
https://doi.org/10.1053/j.gastro.2013.02.042 |
[1, 4]
. Recent systematic analyses have further reinforced the global heterogeneity in definitions and outcomes of ACLF
| [2] | Aggarwal, A., Biswas, S., Arora, U., Vaishnav, M., Shenoy, A., Swaroop, S., Agarwal, A., Elhence, A., Kumar, R., Goel, A., & Shalimar (2024). Definitions, Etiologies, and Outcomes of Acute on Chronic Liver Failure: A Systematic Review and Meta-analysis. Clinical gastroenterology and hepatology: the official clinical practice journal of the American Gastroenterological Association, 22(11), 2199–2210. e25.
https://doi.org/10.1016/j.cgh.2024.04.018 |
[2]
. This heterogeneity was reflected in the present study by the high rate of adverse short-term outcomes observed among hospitalized patients. Our study evaluated the clinical profile of patients with ACLF, their hospital outcomes, and the association between clinical and biochemical parameters and short-term prognosis, providing insight into disease patterns in a North Indian tertiary care setting.
4.2. Demographic Profile of the Study Population
The mean age of patients in this study was 49.96 ± 11.30 years, which is consistent with previous Indian studies and confirms that ACLF predominantly affects individuals in the fourth and fifth decades of life
| [1] | Jalan R, Gines P, Olson JC, Mookerjee RP, Moreau R, Garcia-Tsao G, et al. Acute-on-chronic liver failure. Journal of Hepatology. 2012; 57(6): 1336–1348. https://doi.org/10.1016/j.jhep.2012.06.026 |
| [8] | Shalimar, Saraswat V, Singh SP, Duseja A, Shukla A, Eapen CE, et al. Acute-on-chronic liver failure in India: the Indian National Association for Study of the Liver consortium experience. Journal of Gastroenterology and Hepatology. 2016; 31(10): 1742–1749. https://doi.org/10.1111/jgh.13313 |
[1, 8]
. Shalimar et al. reported similar mean ages ranging from 45 to 50 years, indicating that ACLF affects a relatively younger population in Asia compared with Western cohorts
| [8] | Shalimar, Saraswat V, Singh SP, Duseja A, Shukla A, Eapen CE, et al. Acute-on-chronic liver failure in India: the Indian National Association for Study of the Liver consortium experience. Journal of Gastroenterology and Hepatology. 2016; 31(10): 1742–1749. https://doi.org/10.1111/jgh.13313 |
[8]
. This younger age at presentation highlights the significant socioeconomic burden of ACLF in the Indian setting and may be attributed to earlier onset of alcohol consumption, higher prevalence of viral hepatitis, and increasing metabolic comorbidities.
A marked male predominance (84%) was observed in our cohort, comparable to regional data reporting male proportions of 70–90% among ACLF patients. This finding is largely explained by higher alcohol consumption rates among men. In contrast, Western studies report a relatively lower male predominance, possibly reflecting differences in alcohol use patterns, healthcare access, and etiological profiles
.
4.3. Etiology of Chronic Liver Disease and Precipitating Events
Alcohol was the most common underlying etiology of chronic liver disease in our study, followed by metabolic dysfunction–associated steatohepatitis, hepatitis B virus infection, cryptogenic cirrhosis, and hepatitis C virus infection. These findings are consistent with reports from the INASL ACLF Consortium, which identify alcohol as the leading cause of chronic liver disease in South and Southeast Asia
| [8] | Shalimar, Saraswat V, Singh SP, Duseja A, Shukla A, Eapen CE, et al. Acute-on-chronic liver failure in India: the Indian National Association for Study of the Liver consortium experience. Journal of Gastroenterology and Hepatology. 2016; 31(10): 1742–1749. https://doi.org/10.1111/jgh.13313 |
[8]
. Similar trends have been observed by Shalimar et al., whereas Western studies demonstrate a higher prevalence of metabolic dysfunction–associated steatotic liver disease and hepatitis C virus infection, highlighting significant geographic variability in liver disease epidemiology
| [8] | Shalimar, Saraswat V, Singh SP, Duseja A, Shukla A, Eapen CE, et al. Acute-on-chronic liver failure in India: the Indian National Association for Study of the Liver consortium experience. Journal of Gastroenterology and Hepatology. 2016; 31(10): 1742–1749. https://doi.org/10.1111/jgh.13313 |
| [12] | Asrani SK, O’Leary JG. Acute-on-chronic liver failure. Clinical Liver Disease. 2014; 18(3): 561–574.
https://doi.org/10.1016/j.cld.2014.05.004 |
[8, 12]
.
Alcoholic hepatitis and sepsis were the most common acute precipitating events in the present study. This observation mirrors findings by Jalan et al., who identified sepsis as a critical precipitant associated with systemic inflammation and multiorgan dysfunction
. These precipitating events are known to trigger an exaggerated inflammatory response, thereby accelerating hepatic decompensation and promoting extrahepatic organ failure.
4.4. Clinical Presentation and Complications
Jaundice, abdominal distension, altered sensorium, and abdominal pain were the most frequent presenting symptoms in this study, consistent with APASL guidelines that identify jaundice and ascites as hallmark features of ACLF
| [3] | Sarin SK, Kumar A, Almeida JA, Chawla YK, Fan ST, Garg H, et al. Acute-on-chronic liver failure: consensus recommendations of the Asian Pacific Association for the Study of the Liver. Hepatology International. 2009; 3(1): 269–282.
https://doi.org/10.1007/s12072-008-9106-x |
[3]
. Nearly half of the patients presented with altered sensorium suggestive of hepatic encephalopathy, a prevalence comparable to that reported in Indian studies where hepatic encephalopathy has been documented in 40–60% of ACLF cases
| [8] | Shalimar, Saraswat V, Singh SP, Duseja A, Shukla A, Eapen CE, et al. Acute-on-chronic liver failure in India: the Indian National Association for Study of the Liver consortium experience. Journal of Gastroenterology and Hepatology. 2016; 31(10): 1742–1749. https://doi.org/10.1111/jgh.13313 |
[8]
. Fever was observed in a substantial proportion of patients, supporting the role of infection-related triggers in ACLF pathogenesis
| [3] | Sarin SK, Kumar A, Almeida JA, Chawla YK, Fan ST, Garg H, et al. Acute-on-chronic liver failure: consensus recommendations of the Asian Pacific Association for the Study of the Liver. Hepatology International. 2009; 3(1): 269–282.
https://doi.org/10.1007/s12072-008-9106-x |
| [4] | Moreau R, Jalan R, Gines P, Pavesi M, Angeli P, Cordoba J, et al. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology. 2013; 144(7): 1426–1437.
https://doi.org/10.1053/j.gastro.2013.02.042 |
[3, 4]
.
Ascites was almost universal in our cohort, while portal hypertension and hepatic encephalopathy were also highly prevalent. Importantly, hepatic encephalopathy showed a statistically significant association with poor outcomes. This finding is consistent with the CANONIC study, which identified hepatic encephalopathy as a strong predictor of mortality in ACLF, underscoring its value as an important prognostic marker
| [4] | Moreau R, Jalan R, Gines P, Pavesi M, Angeli P, Cordoba J, et al. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology. 2013; 144(7): 1426–1437.
https://doi.org/10.1053/j.gastro.2013.02.042 |
[4]
.
4.5. Laboratory Parameters and Prognostic Indicators
Several laboratory parameters demonstrated significant associations with adverse outcomes. Elevated international normalized ratio and prolonged prothrombin time reflected severe hepatic synthetic dysfunction and were strongly associated with mortality. Leukocytosis was more common among non-survivors, reinforcing the contribution of sepsis and systemic inflammation to disease severity
| [1] | Jalan R, Gines P, Olson JC, Mookerjee RP, Moreau R, Garcia-Tsao G, et al. Acute-on-chronic liver failure. Journal of Hepatology. 2012; 57(6): 1336–1348. https://doi.org/10.1016/j.jhep.2012.06.026 |
| [4] | Moreau R, Jalan R, Gines P, Pavesi M, Angeli P, Cordoba J, et al. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology. 2013; 144(7): 1426–1437.
https://doi.org/10.1053/j.gastro.2013.02.042 |
[1, 4]
.
Higher serum bilirubin was significantly associated with mortality, indicating severe cholestasis and hepatocellular injury. These findings are consistent with observations by Shalimar et al., suggesting that these parameters serve as easily measurable markers for early risk stratification in ACLF
| [8] | Shalimar, Saraswat V, Singh SP, Duseja A, Shukla A, Eapen CE, et al. Acute-on-chronic liver failure in India: the Indian National Association for Study of the Liver consortium experience. Journal of Gastroenterology and Hepatology. 2016; 31(10): 1742–1749. https://doi.org/10.1111/jgh.13313 |
[8]
. Hyperkalemia emerged as an important predictor of poor outcome, reflecting advanced renal dysfunction and impaired electrolyte handling. Serum creatinine, ammonia, and lactate levels also showed strong associations with adverse outcomes. Renal dysfunction is a well-established determinant of mortality in ACLF
| [4] | Moreau R, Jalan R, Gines P, Pavesi M, Angeli P, Cordoba J, et al. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology. 2013; 144(7): 1426–1437.
https://doi.org/10.1053/j.gastro.2013.02.042 |
[4]
, while elevated ammonia correlates with the severity of hepatic encephalopathy. Elevated lactate reflects tissue hypoxia, circulatory dysfunction, and severe inflammation, all of which predict multiorgan failure and mortality
| [4] | Moreau R, Jalan R, Gines P, Pavesi M, Angeli P, Cordoba J, et al. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology. 2013; 144(7): 1426–1437.
https://doi.org/10.1053/j.gastro.2013.02.042 |
[4]
.
4.6. Severity Scores and Predictors of Mortality
Child–Turcotte–Pugh, Model for End-Stage Liver Disease, and MELD-Na scores were significantly higher among non-survivors, confirming their role as important predictors of mortality in ACLF. Among these, MELD-Na demonstrated superior prognostic performance. The strong correlation between elevated MELD-Na scores and mortality in our study reinforces its value as a practical and reliable tool for risk stratification, clinical decision-making, and prioritization for advanced therapies
| [9] | Zhang Q, Guo X, Zhao S, Pang X, Wang Y, Zhang Y, Chi B. Prognostic performance of clinical indices and model scorings for acute-on-chronic liver failure: a study of 164 patients. Experimental and Therapeutic Medicine. 2016; 11(4): 1348–1354. https://doi.org/10.3892/etm.2016.3037 |
[9]
. Predictors of mortality identified on univariate analysis included the presence of hepatic encephalopathy, elevated INR, serum creatinine, serum potassium, ammonia, lactate levels, and high MELD and MELD-Na scores. These findings support the pathophysiological framework proposed by Moreau et al. and Jalan et al., which describes ACLF as a syndrome driven by excessive systemic inflammation, circulatory dysfunction, mitochondrial failure, and progressive multiorgan failure
| [1] | Jalan R, Gines P, Olson JC, Mookerjee RP, Moreau R, Garcia-Tsao G, et al. Acute-on-chronic liver failure. Journal of Hepatology. 2012; 57(6): 1336–1348. https://doi.org/10.1016/j.jhep.2012.06.026 |
| [4] | Moreau R, Jalan R, Gines P, Pavesi M, Angeli P, Cordoba J, et al. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology. 2013; 144(7): 1426–1437.
https://doi.org/10.1053/j.gastro.2013.02.042 |
[1, 4]
.
4.7. Comparison with Previous Studies
Our findings are consistent with those of Shalimar et al. from the APASL ACLF Consortium, who reported alcohol as the most common etiology of ACLF with a high prevalence of hepatic encephalopathy
| [8] | Shalimar, Saraswat V, Singh SP, Duseja A, Shukla A, Eapen CE, et al. Acute-on-chronic liver failure in India: the Indian National Association for Study of the Liver consortium experience. Journal of Gastroenterology and Hepatology. 2016; 31(10): 1742–1749. https://doi.org/10.1111/jgh.13313 |
[8]
. The CANONIC study by Moreau et al. identified organ failure, particularly renal dysfunction, as the strongest predictor of mortality, a finding supported by our results
| [4] | Moreau R, Jalan R, Gines P, Pavesi M, Angeli P, Cordoba J, et al. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology. 2013; 144(7): 1426–1437.
https://doi.org/10.1053/j.gastro.2013.02.042 |
[4]
. Jalan et al. described ACLF as a systemic inflammatory syndrome with circulatory and multiorgan failure, aligning with the association between elevated lactate levels and mortality observed in our cohort
. The in-hospital mortality rate of 46% in our study is comparable to the 35–55% mortality reported in Indian ACLF cohorts by Shalimar et al.
| [8] | Shalimar, Saraswat V, Singh SP, Duseja A, Shukla A, Eapen CE, et al. Acute-on-chronic liver failure in India: the Indian National Association for Study of the Liver consortium experience. Journal of Gastroenterology and Hepatology. 2016; 31(10): 1742–1749. https://doi.org/10.1111/jgh.13313 |
[8]
. Additionally, Zhang et al. demonstrated the superiority of MELD-Na over MELD for mortality prediction in ACLF, a finding reaffirmed in the present study
| [9] | Zhang Q, Guo X, Zhao S, Pang X, Wang Y, Zhang Y, Chi B. Prognostic performance of clinical indices and model scorings for acute-on-chronic liver failure: a study of 164 patients. Experimental and Therapeutic Medicine. 2016; 11(4): 1348–1354. https://doi.org/10.3892/etm.2016.3037 |
[9]
.
4.8. Clinical Implications, Limitations, and Future Directions
Early identification of high-risk features such as elevated INR, serum creatinine, ammonia, lactate, and MELD-Na scores can facilitate timely intensive monitoring, prompt management of precipitating events, and early referral for liver transplantation. MELD-Na should be preferred over MELD alone for prognostication in ACLF. Preventive strategies, including early infection screening, timely antimicrobial therapy, alcohol cessation programs, nutritional optimization, and adult immunization against preventable infections, are essential components of comprehensive ACLF management.
This study has certain limitations. It was conducted at a single tertiary care center with a relatively small sample size, which may limit the generalizability of the findings. The limited number of mortality events restricted the ability to perform multivariate regression analysis; therefore, associations with in-hospital mortality are based on univariate analysis and interpreted cautiously. Consequently, the study may have been underpowered to identify independent prognostic predictors.
In addition, inflammatory biomarkers and advanced ACLF grading systems such as CLIF-SOFA were not systematically evaluated. Dynamic changes in clinical and laboratory parameters during hospitalization were also not assessed.
Future multicenter prospective studies with larger cohorts are required to validate these findings, establish independent predictors of mortality, evaluate temporal trends in prognostic parameters, assess long-term outcomes, and explore the role of inflammatory biomarkers in improving risk stratification. Recent advances in prognostic modeling and extracorporeal liver support systems warrant further evaluation in larger cohorts to determine their impact on survival outcomes in ACLF
| [10] | Shen, Y., Xu, W., Chen, Y. et al. Early prediction of acute-on-chronic liver failure development in patients with diverse chronic liver diseases. Sci Rep 14, 28245 (2024).
https://doi.org/10.1038/s41598-024-79486-w |
| [11] | Agarwal, B., Cañizares, R. B., Saliba, F., Ballester, M. P., Tomescu, D. R., Martin, D., Stadlbauer, V., Wright, G., Sheikh, M., Morgan, C., Alzola, C., Lavin, P., Green, D., Kumar, R., Sacleux, S. C., Schilcher, G., Koball, S., Tudor, A., Minten, J., Domenech, G., … Jalan, R. (2023). Randomized, controlled clinical trial of the DIALIVE liver dialysis device versus standard of care in patients with acute-on- chronic liver failure. Journal of hepatology, 79(1), 79–92.
https://doi.org/10.1016/j.jhep.2023.03.013 |
[10, 11]
. Strengthening early liver transplantation referral pathways may further improve survival outcomes in patients with ACLF.
5. Conclusions
Acute-on-chronic liver failure in a tertiary care setting predominantly affects middle-aged males with alcohol-related chronic liver disease, with alcoholic hepatitis and sepsis being the most common precipitating events. The condition is characterized by severe multisystem involvement and is associated with high in-hospital mortality. Laboratory parameters reflecting hepatic synthetic dysfunction, renal impairment, metabolic derangements, and circulatory failure—including elevated international normalized ratio, serum creatinine, ammonia, lactate, and serum potassium levels—as well as higher MELD and MELD-Na scores, were significantly associated with poor outcomes. Hepatic encephalopathy emerged as the most significant clinical complication associated with mortality on univariate analysis. Early recognition of high-risk patients, aggressive management of precipitating factors, timely escalation of supportive care, and prompt evaluation for liver transplantation are crucial to improving short-term outcomes in patients with acute-on-chronic liver failure.
Abbreviations
ACLF | Acute-on-Chronic Liver Failure |
CLD | Chronic Liver Disease |
APASL | Asian Pacific Association for the Study of the Liver |
EASL | European Association for the Study of the Liver |
AASLD | American Association for the Study of Liver Diseases |
CLIF | Chronic Liver Failure |
NACSELD | North American Consortium for the Study of End-Stage Liver Disease |
CTP | Child–Turcotte–Pugh |
MELD | Model for End-Stage Liver Disease |
MELD-Na | Model for End-Stage Liver Disease–Sodium |
INR | International Normalized Ratio |
HCC | Hepatocellular Carcinoma |
HBV | Hepatitis B Virus |
HCV | Hepatitis C Virus |
MASLD | Metabolic Dysfunction–Associated Steatotic Liver Disease |
MASH | Metabolic Dysfunction–Associated Steatohepatitis |
SBP | Spontaneous Bacterial Peritonitis |
Author Contributions
Shreyansh Goyal: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Validation, Visualization, Writing – original draft
Prabhat Sinha: Supervision
Sharad Malhotra: Supervision
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Jalan R, Gines P, Olson JC, Mookerjee RP, Moreau R, Garcia-Tsao G, et al. Acute-on-chronic liver failure. Journal of Hepatology. 2012; 57(6): 1336–1348.
https://doi.org/10.1016/j.jhep.2012.06.026
|
| [2] |
Aggarwal, A., Biswas, S., Arora, U., Vaishnav, M., Shenoy, A., Swaroop, S., Agarwal, A., Elhence, A., Kumar, R., Goel, A., & Shalimar (2024). Definitions, Etiologies, and Outcomes of Acute on Chronic Liver Failure: A Systematic Review and Meta-analysis. Clinical gastroenterology and hepatology: the official clinical practice journal of the American Gastroenterological Association, 22(11), 2199–2210. e25.
https://doi.org/10.1016/j.cgh.2024.04.018
|
| [3] |
Sarin SK, Kumar A, Almeida JA, Chawla YK, Fan ST, Garg H, et al. Acute-on-chronic liver failure: consensus recommendations of the Asian Pacific Association for the Study of the Liver. Hepatology International. 2009; 3(1): 269–282.
https://doi.org/10.1007/s12072-008-9106-x
|
| [4] |
Moreau R, Jalan R, Gines P, Pavesi M, Angeli P, Cordoba J, et al. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology. 2013; 144(7): 1426–1437.
https://doi.org/10.1053/j.gastro.2013.02.042
|
| [5] |
Jalan R, Yurdaydin C, Bajaj JS, Acharya SK, Arroyo V, Lin H-C, et al. Toward an improved definition of acute-on-chronic liver failure. Gastroenterology. 2014; 147(1): 4–10.
https://doi.org/10.1053/j.gastro.2014.05.005
|
| [6] |
Sarin SK, Choudhury A. Acute-on-chronic liver failure: terminology, mechanisms and management. Nature Reviews Gastroenterology & Hepatology. 2016; 13: 131–149.
https://doi.org/10.1038/nrgastro.2015.219
|
| [7] |
Verbeke L, Nevens F, Laleman W. Bench-to-bedside review: acute-on-chronic liver failure—linking the gut, liver and systemic circulation. Critical Care. 2011; 15: 233.
https://doi.org/10.1186/cc10424
|
| [8] |
Shalimar, Saraswat V, Singh SP, Duseja A, Shukla A, Eapen CE, et al. Acute-on-chronic liver failure in India: the Indian National Association for Study of the Liver consortium experience. Journal of Gastroenterology and Hepatology. 2016; 31(10): 1742–1749.
https://doi.org/10.1111/jgh.13313
|
| [9] |
Zhang Q, Guo X, Zhao S, Pang X, Wang Y, Zhang Y, Chi B. Prognostic performance of clinical indices and model scorings for acute-on-chronic liver failure: a study of 164 patients. Experimental and Therapeutic Medicine. 2016; 11(4): 1348–1354.
https://doi.org/10.3892/etm.2016.3037
|
| [10] |
Shen, Y., Xu, W., Chen, Y. et al. Early prediction of acute-on-chronic liver failure development in patients with diverse chronic liver diseases. Sci Rep 14, 28245 (2024).
https://doi.org/10.1038/s41598-024-79486-w
|
| [11] |
Agarwal, B., Cañizares, R. B., Saliba, F., Ballester, M. P., Tomescu, D. R., Martin, D., Stadlbauer, V., Wright, G., Sheikh, M., Morgan, C., Alzola, C., Lavin, P., Green, D., Kumar, R., Sacleux, S. C., Schilcher, G., Koball, S., Tudor, A., Minten, J., Domenech, G., … Jalan, R. (2023). Randomized, controlled clinical trial of the DIALIVE liver dialysis device versus standard of care in patients with acute-on- chronic liver failure. Journal of hepatology, 79(1), 79–92.
https://doi.org/10.1016/j.jhep.2023.03.013
|
| [12] |
Asrani SK, O’Leary JG. Acute-on-chronic liver failure. Clinical Liver Disease. 2014; 18(3): 561–574.
https://doi.org/10.1016/j.cld.2014.05.004
|
| [13] |
Bajaj JS, et al. Acute-on-chronic liver failure defined by North American Consortium for the Study of End-Stage Liver Disease criteria. Hepatology. 2014; 60(6): 1853–1861.
https://doi.org/10.1002/hep.27323
|
| [14] |
Choudhury, A., Kulkarni, A. V., Arora, V. et al. Acute-on-chronic liver failure (ACLF): the ‘Kyoto Consensus’—steps from Asia. Hepatol Int 19, 1–69 (2025).
https://doi.org/10.1007/s12072-024-10773-4
|
Cite This Article
-
APA Style
Goyal, S., Sinha, P., Malhotra, S. (2026). Clinical Profile and Predictors of Hospital Outcomes in Acute-on-chronic Liver Failure. International Journal of Gastroenterology, 10(1), 9-19. https://doi.org/10.11648/j.ijg.20261001.13
 Copy
|
Copy
|
 Download
Download
ACS Style
Goyal, S.; Sinha, P.; Malhotra, S. Clinical Profile and Predictors of Hospital Outcomes in Acute-on-chronic Liver Failure. Int. J. Gastroenterol. 2026, 10(1), 9-19. doi: 10.11648/j.ijg.20261001.13
Copy
|
Download
AMA Style
Goyal S, Sinha P, Malhotra S. Clinical Profile and Predictors of Hospital Outcomes in Acute-on-chronic Liver Failure. Int J Gastroenterol. 2026;10(1):9-19. doi: 10.11648/j.ijg.20261001.13
Copy
|
Download
-
@article{10.11648/j.ijg.20261001.13,
author = {Shreyansh Goyal and Prabhat Sinha and Sharad Malhotra},
title = {Clinical Profile and Predictors of Hospital Outcomes in Acute-on-chronic Liver Failure},
journal = {International Journal of Gastroenterology},
volume = {10},
number = {1},
pages = {9-19},
doi = {10.11648/j.ijg.20261001.13},
url = {https://doi.org/10.11648/j.ijg.20261001.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijg.20261001.13},
abstract = {Acute-on-chronic liver failure (ACLF) is a distinct clinical syndrome characterized by acute hepatic deterioration in patients with underlying chronic liver disease and is associated with multiorgan dysfunction and high short-term mortality. In India, alcohol remains the predominant etiology of chronic liver disease, with infectious causes and alcoholic hepatitis being common acute precipitating events. However, clinical profiles and predictors of in-hospital outcomes show variability across populations. This hospital-based observational study included 50 patients diagnosed with ACLF according to the APASL criteria and admitted to Aakash Healthcare Super Speciality Hospital, New Delhi, between February 2024 and January 2026. Detailed clinical evaluation and laboratory investigations were performed at admission. Disease severity was assessed using Child–Turcotte–Pugh, Model for End-Stage Liver Disease (MELD), and MELD-Na scores. Precipitating factors, complications, organ system involvement, and outcomes during hospitalization were documented. Outcomes were categorized as survival with discharge, in-hospital mortality, or referral for liver transplantation. The mean age of patients was 49.96 ± 11.30 years, with a male predominance (84%). Alcohol-related liver disease was the most common underlying etiology (60%). Alcoholic hepatitis (38%) and sepsis (30%) were the leading precipitating events. Jaundice, abdominal distension, and altered sensorium were the most frequent presenting symptoms. Ascites (96%), portal hypertension (92%), and hepatic encephalopathy (78%) were the predominant complications. In-hospital mortality was observed in 46% of patients, while 22% required referral for liver transplantation. Elevated international normalized ratio, serum creatinine, ammonia, lactate, serum potassium levels, and higher MELD and MELD-Na scores were significantly associated with poor outcomes (p < 0.05). Hepatic encephalopathy was the only clinical complication significantly associated with mortality on univariate analysis (p = 0.021). ACLF predominantly affects middle-aged males with alcohol-related chronic liver disease and is associated with high in-hospital mortality. Early identification of high-risk patients and timely escalation of care, including prompt evaluation for liver transplantation, are crucial to improving outcomes.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Clinical Profile and Predictors of Hospital Outcomes in Acute-on-chronic Liver Failure
AU - Shreyansh Goyal
AU - Prabhat Sinha
AU - Sharad Malhotra
Y1 - 2026/03/19
PY - 2026
N1 - https://doi.org/10.11648/j.ijg.20261001.13
DO - 10.11648/j.ijg.20261001.13
T2 - International Journal of Gastroenterology
JF - International Journal of Gastroenterology
JO - International Journal of Gastroenterology
SP - 9
EP - 19
PB - Science Publishing Group
SN - 2640-169X
UR - https://doi.org/10.11648/j.ijg.20261001.13
AB - Acute-on-chronic liver failure (ACLF) is a distinct clinical syndrome characterized by acute hepatic deterioration in patients with underlying chronic liver disease and is associated with multiorgan dysfunction and high short-term mortality. In India, alcohol remains the predominant etiology of chronic liver disease, with infectious causes and alcoholic hepatitis being common acute precipitating events. However, clinical profiles and predictors of in-hospital outcomes show variability across populations. This hospital-based observational study included 50 patients diagnosed with ACLF according to the APASL criteria and admitted to Aakash Healthcare Super Speciality Hospital, New Delhi, between February 2024 and January 2026. Detailed clinical evaluation and laboratory investigations were performed at admission. Disease severity was assessed using Child–Turcotte–Pugh, Model for End-Stage Liver Disease (MELD), and MELD-Na scores. Precipitating factors, complications, organ system involvement, and outcomes during hospitalization were documented. Outcomes were categorized as survival with discharge, in-hospital mortality, or referral for liver transplantation. The mean age of patients was 49.96 ± 11.30 years, with a male predominance (84%). Alcohol-related liver disease was the most common underlying etiology (60%). Alcoholic hepatitis (38%) and sepsis (30%) were the leading precipitating events. Jaundice, abdominal distension, and altered sensorium were the most frequent presenting symptoms. Ascites (96%), portal hypertension (92%), and hepatic encephalopathy (78%) were the predominant complications. In-hospital mortality was observed in 46% of patients, while 22% required referral for liver transplantation. Elevated international normalized ratio, serum creatinine, ammonia, lactate, serum potassium levels, and higher MELD and MELD-Na scores were significantly associated with poor outcomes (p < 0.05). Hepatic encephalopathy was the only clinical complication significantly associated with mortality on univariate analysis (p = 0.021). ACLF predominantly affects middle-aged males with alcohol-related chronic liver disease and is associated with high in-hospital mortality. Early identification of high-risk patients and timely escalation of care, including prompt evaluation for liver transplantation, are crucial to improving outcomes.
VL - 10
IS - 1
ER -
Copy
|
Download