Abstract
Introduction: Antenatal corticosteroid therapy reduces the risk of developing RDS in premature infants. A single complete course of two doses of betamethasone is recommended between 24 weeks and 34 weeks. There are few data on the neonatal effects of an incomplete course of antenatal corticosteroid therapy. The main objective of our study is to evaluate the effectiveness of a complete versus incomplete course of antenatal corticosteroid therapy on the number of doses of surfactant received postnatally. Methods: This is a single-center retrospective study, including 145 newborns with RDS, divided into 2 groups according to the number of doses of antenatal corticosteroid therapy (1 dose; n = 23 and 2 doses; n = 95). Results: The clinical characteristics of the newborns were similar in the 2 groups. The number of doses of surfactants received postnatally and the severity of RDS are not influenced by the number of doses of antenatal corticosteroid therapy. On the other hand, the number of doses of surfactants received is influenced by the term of birth, the presence of an neonatal sepsis and by resuscitation in the delivery room. The severity of RDS is not influenced either by the interval between the last dose of antenatal corticosteroid therapy and delivery, nor by the cause of prematurity. We did not note any statistically significant difference in clinical improvement (duration of intubation, duration of non-invasive ventilation), the need for postnatal corticosteroid therapy and the risk of occurrence of morbidity and mortality (mortality rate, occurrence of BPD, IVH, severe NEC) between the two groups. Conclusion: just like a complete course, an incomplete course of antenatal corticosteroid therapy can also act on the severity of RDS. Prospective randomized studies should be considered for a formal determination of the neonatal effects of a complete versus incomplete course of antenatal corticosteroid therapy, including the trial BETADOSE.
Keywords
Antenatal Corticosteroid Therapy, Surfactant, Dose, RDS, BPD
1. Introduction
Preterm delivery is associated with neonatal mortality and severe morbidity, including hyaline membrane disease, intraventricular hemorrhage, necrotizing enterocolitis, neonatal sepsis, retinopathy of prematurity, and bronchopulmonary dysplasia
| [1] | Simonetta Costa, Enrico Zecca, Daniele De Luca, Maria Pia De Carolis, Costantino Romagnoli. Efficacy of a single dose of antenatal corticosteroids on morbidity and mortality of preterm infants. Eur J Obstet Gynecol Reprod Biol. 2007 Apr; 131(2): 154-7. |
[1]
.
RDS is a serious respiratory pathology due to surfactant deficiency, the incidence of which is inversely proportional to gestational age. In the absence of fetal lung maturation with corticosteroids, its incidence is approximately 60% in newborns with gestational age less than 30 weeks and almost 100% in those less than 26 weeks
| [2] | Saliba E. Néonatalogie: bases scientifiques. 2017. (Elsevier Masson). |
[2]
.
Antenatal administration of corticosteroids to pregnant women at risk of preterm delivery reduces the risk of developing RDS in premature infants, increases the effectiveness of surfactant therapy and significantly reduces the risk of IVH and mortality by more than 40%
| [1] | Simonetta Costa, Enrico Zecca, Daniele De Luca, Maria Pia De Carolis, Costantino Romagnoli. Efficacy of a single dose of antenatal corticosteroids on morbidity and mortality of preterm infants. Eur J Obstet Gynecol Reprod Biol. 2007 Apr; 131(2): 154-7. |
[1]
.
A single course of corticosteroids is recommended for pregnant women between 24 and 34 weeks gestation who are at risk of premature birth. This treatment is associated in the neonatal period with a significant reduction in RDS, IVH, NEC and death
| [3] | The American College of Obstetrics and Gynecology. Antenatal Corticosteroid Therapy for Fetal Maturation. Committee Opinion, Number 713, August 2017. |
[3]
.
Betamethasone is recommended as the steroid of choice, to be administered in two doses of 12 mg IM 24 hours apart
| [4] | Xavier Miracle, Gian Carlo Di Renzo, Ann Stark, Avroy Fanaroff, Xavier Carbonell-Estrany, Erich Saling. Guideline for the use of antenatal corticosteroids for fetal maturation. J. Perinat. Med. 36(2008) 191–196. |
[4]
.
The beneficial effects of a complete course of antenatal corticosteroid therapy are greatest if more than 24 hours and less than 7 days have elapsed between the last dose of corticosteroid therapy and delivery
| [1] | Simonetta Costa, Enrico Zecca, Daniele De Luca, Maria Pia De Carolis, Costantino Romagnoli. Efficacy of a single dose of antenatal corticosteroids on morbidity and mortality of preterm infants. Eur J Obstet Gynecol Reprod Biol. 2007 Apr; 131(2): 154-7. |
[1]
.
However, premature birth is often unpredictable, and may be unavoidable; it is sometimes induced for maternal or fetal indications, before the end of corticosteroid therapy. There are few data on the neonatal effects of an incomplete cycle of antenatal corticosteroid therapy
| [5] | Seger N, Soll R. Animal derived surfactant extract for treatment of respiratory distress syndrome. Cochrane Database Syst Rev. 2009; (2): CD007836. PMID: 19370695 https://doi.org/10.1002/14651858.CD007836 |
| [6] | Sen S, Reghu A, Ferguson SD. Efficacy of a single dose of antenatal steroid in surfactant-treated babies under 31 weeks’ gestation. JMatern Fetal Neonatal Med 2002; 12: 298–303. PMID: 12607761 https://doi.org/10.1080/jmf.12.5.298.303 |
[5, 6]
. Our retrospective study of 145 newborns at the NOVO Hospital in Pontoise aims to evaluate the impact of the number of doses of antenatal corticosteroid therapy on the number of doses of postnatal surfactant.
2. Patients and Methods
2.1. Type and Population of the Study: (Figure 1)
The study took place in the Neonatal Intensive Care Unit at the NOVO Hospital center in Pontoise, France.
We conducted a retrospective, single-center study, including all premature infants less than 37 weeks old with RDS, numbering 145, between January 2018 and December 2019. The patients were divided into 2 groups according to the number of doses of antenatal corticosteroid therapy administered:
1) Group 1 (23 newborns): 1 dose of antenatal corticosteroid therapy: incomplete course
2) Group 2 (95 newborns): 2 doses of antenatal corticosteroid therapy: complete course
We excluded from the study:
1) Newborns suffering from serious congenital malformations (4 patients).
2) Newborns who did not receive antenatal corticosteroid therapy (23 patients).
2.2. Objectives of the Study
To date, no study has demonstrated that the administration of two doses of betamethasone antenatally is more effective than that of a single dose, in lung maturation and prevention of RDS.
The main objective of our study is to evaluate, in a cohort of 145 premature infants treated for RDS, the effectiveness of a complete course versus an incomplete course of antenatal corticosteroid therapy, on the number of doses of postnatal surfactant.
Our secondary objectives are:
1) Observe the influence of gestational age on the severity of RDS.
2) Observe the influence of the cause of prematurity on the severity of RDS.
3) Observe the impact of the interval between the last dose of antenatal corticosteroid therapy and birth on the severity of RDS.
4) Observe the impact of the number of doses of antenatal corticosteroid therapy on the use of postnatal corticosteroid therapy.
5) Observe the impact of the number of doses of antenatal corticosteroid therapy on the prevalence of bronchopulmonary dysplasia.
6) Observe the impact of the number of doses of antenatal corticosteroid therapy on the severity of intraventricular hemorrhage.
2.3. Materials and Methods
Data collection was based on computerized medical records, prescription and hourly monitoring sheets, and radiological examinations.
Parents were informed of the use of their child's medical data for research purposes. The study complies with the CNIL reference methodology MR-004, whose declaration number is: 2213337 v 0.
We recorded the following data for the 145 newborns:
1) epidemiological data: gestational age, sex, route of delivery, etc.
2) clinical data: birth weight, IUGR, etc.
3) paraclinical data: biology, radiological stages of RDS
4) treatment: resuscitation in the delivery room, surfactant instillation method, number of surfactant doses received, post-natal corticosteroid therapy, etc.
5) evolution: clinical improvement, complication (BPD, IVH, severe NEC), death.
2.4. Statistical Analyses
The data entry and statistical analysis was carried out using Excel 2016 and the R software. The statistical analysis consists of calculating the medians, means, standard deviations and the p-value. A p-value < 0.05 was considered statistically significant. Discrete data were presented as percentages then compared using Pearson's Χ2 test with Yates correction if necessary. The numerical data were presented by their median then compared using the non-parametric Wilcoxon test. The multivariate analysis was carried out using logistic regression.
3. Results
3.1. Epidemiological Data
a- Frequency:
During the period from 1st of January 2018 to 31 December 2019, 9613 births were recorded at the NOVO Hopspital, including 1095 newborns hospitalized in the neonatal intensive care unit. Among these patients, 145 cases presented with RDS, an incidence of 13%.
b- Distribution of patients according to years, sex and term:
74 patients (52%) who presented with RDS were collected during 2019 compared to 71 patients (48%) in 2018. The M/F sex ratio was 1.23 (80 boys and 65 girls).
The average term of birth of the patients was 28 ± 3 weeks of amenorrhea, with extremes ranging from 24 to 37 weeks.
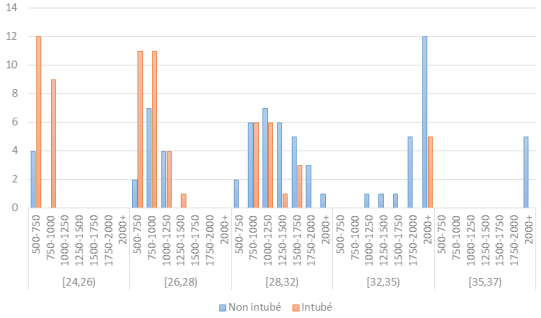
3.2. Clinical Characteristics of Patients (Table 1) (Figure 2)
The clinical characteristics of the newborns were similar in the 2 groups (sex ratio, gestational age, birth weight, IUGR, resuscitation in the delivery room, and umbilical cord ph and lactate at birth, etc.). In a multivariate analysis, birth weight was not significantly associated with the risk of intubation in the delivery room (OR=1.00024; p=0.057), unlike gestational age (OR=0.88; p<0.001) with a reduced risk of intubation by 12% per additional week of gestation.
Figure 2. Number of Newborns Intubated in the Delivery Room according to Birth Weight and Gestational Age.
Table 1. Clinical characteristics of neonates.
| Corticoïdes antenatal | |
| Total, N=118 | Demidose, N=23 | Pleine dose, N = 95 | p-value |
Sexe | | | | 0.2 |
F | 54 (46%) | 8 (35%) | 46 (48%) | |
H | 64 (54%) | 15 (65%) | 49 (52%) | |
Cause.prematurite | | | | 0.8 |
spontanée | 66 (56%) | 14 (61%) | 52 (55%) | |
ARCF | 16 (14%) | 3 (13%) | 13 (14%) | |
Pré éclampsie | 29 (25%) | 4 (17%) | 25 (26%) | |
autre | 7 (5.9%) | 2 (8.7%) | 5 (5.3%) | |
Terme de naissance | | | | 0.093 |
prématurité moyenne | 18 (15%) | 7 (30%) | 11 (12%) | |
grande prématurité | 43 (36%) | 6 (26%) | 37 (39%) | |
très grande prématurité | 57 (48%) | 10 (43%) | 47 (49%) | |
Voie.daccouvhement | | | | 0.3 |
césarienne | 67 (57%) | 11 (48%) | 56 (59%) | |
VB | 51 (43%) | 12 (52%) | 39 (41%) | |
Poids.naissance (g) | 965 (764, 1,410) | 1,110 (835, 1,886) | 935 (728, 1,270) | 0.063 |
RCIU | | | | 0.3 |
non | 99 (84%) | 20 (87%) | 79 (83%) | |
RCIU modéré | 12 (10%) | 2 (8.7%) | 10 (11%) | |
RCIU sévère | 6 (5.1%) | 0 (0%) | 6 (6.3%) | |
IMF | | | | 0.4 |
non | 50 (42%) | 8 (35%) | 42 (44%) | |
Suspectée | 56 (47%) | 11 (48%) | 45 (47%) | |
Confirmée | 12 (10%) | 4 (17%) | 8 (8.4%) | |
Reanimation.en.sdn | | | | 0.9 |
Intubation | 53 (45%) | 10 (45%) | 43 (45%) | |
Intubation+Drogues | 6 (5.1%) | 1 (4.5%) | 5 (5.3%) | |
non | 4 (3.4%) | 0 (0%) | 4 (4.2%) | |
VNI | 54 (46%) | 11 (50%) | 43 (45%) | |
Unknown | 1 | 1 | 0 | |
Ph.au.cordon | 7.28 (7.23, 7.32) | 7.24 (7.14,7.34) | 7.29 (7.24, 7.32) | 0.3 |
Unknown | 11 | 5 | 6 | |
Lactates | 3.20 (2.50, 4.90) | 4.00 (2.60, 7.20) | 3.10 (2.50, 4.40) | 0.2 |
Unknown | 13 | 6 | 7 | |
INSURE | | | | >0.9 |
non | 111 (96%) | 21 (95%) | 90 (96%) | |
oui | 5 (4.3%) | 1 (4.5%) | 4 (4.3%) | |
LISA | | | | >0.9 |
non | 113 (97%) | 22 (100%) | 91 (97%) | |
oui | 3 (2.6%) | 0 (0%) | 3 (3.2%) | |
3.3. Influence of the Number of Doses of Antenatal Corticosteroid on the Number of Doses of Postnatal Surfactant and on the Radiological Severity of RDS
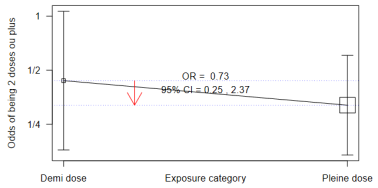
The percentage of patients who required ≥ 2 doses of surfactant in groups 1 and 2 is 30% and 25% respectively, with a statistically insignificant difference (p value 0.596, OR = 0.73, 95% CI = 0.25, 2.37). (
Figures 3 and 4)
Figure 3. Number of postnatal surfactant doses according to the number of antenatal corticosteroid therapy doses.
Figure 4. Odds Ratio of ≥ 2 doses of postnatal surfactant according to the number of doses of antenatal corticosteroid therapy.
The percentage of patients who have RDS grade 3 or 4 in groups 1 and 2 is 48% and 39% respectively, with a statistically insignificant difference (p value 0.4). (
Table 2).
Table 2. Radiological severity of RDS according to the number of doses of antenatal corticosteroid therapy.
| Corticoïdes antenatal | |
| Total, N=118 | Demi dose, N = 23 | Pleine dose, N = 95 | p-value |
Grade Radiologique de la MMH | | | | 0.4 |
MMH 1-2 | 70 (59%) | 12 (52%) | 58 (61%) | |
MMH 3-4 | 48 (41%) | 11 (48%) | 37 (39%) | |
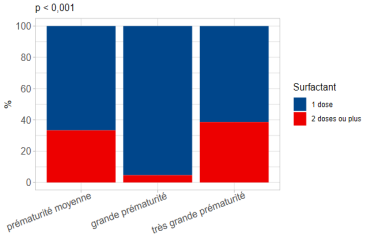
3.4. The Influence of Gestational Age on the Number of Doses of Surfactants
The percentage of patients who received ≥ 2 doses of surfactants is 33% for premature babies between 32 weeks and 37 weeks, 5% for premature babies between 28 weeks and 32 weeks and 38% for premature babies less than 28 weeks; with a statistically significant difference between these 3 groups (p value < 0.01). (
Figure 5).
The majority of patients in both groups required standard intubation for surfactant administration with 96% and 97% in groups 1 and 2 respectively. The rest was done by InSurE method or by LISA (
Table 1).
Figure 5. Number of doses of Postnatal Surfactant Doses according to gestational age.
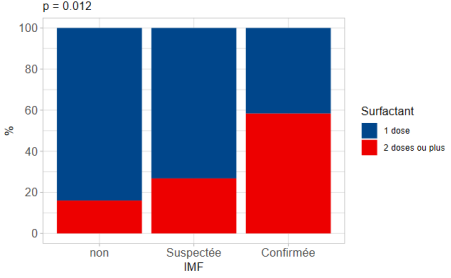
3.5. The Influence of the Neonatal Sepsis on the Number of Doses of Surfactant Received
58% of patients with confirmed neonatal sepsis required ≥ 2 doses of surfactant, compared to 17% of patients with no concept of neonatal sepsis. This difference is statistically significant with a p value of 0.012. (
Figure 6).
Figure 6. Number of Postnatal Surfactant Doses depending on Neonatal Sepsis.
3.6. Resuscitation in the Delivery Room and Number of Doses of Surfactant Received
60% of newborns who were intubated in the delivery room required two or more doses of surfactant, compared to 13% of those who were ventilated with non-invasive ventilation, and 6.7% of those who were not intubated or ventilated. (
Table 3).
Table 3. Delivery Room Resuscitation and Number of Doses of Surfactant.
| Doses de surfactants | |
| Total (N = 118) | 1 dose, N = 88 | ≥2doses, N = 30 | p-value |
reanimation.en.sdn | | | | 0.001 |
Intubation | 51 (44%) | 33 (38%) | 18 (60%) | |
Intubation+Drogues | 6 (5.1%) | 2 (2.3%) | 4 (13%) | |
non | 4 (3.4%) | 2 (2.3%) | 2 (6.7%) | |
VNI | 54 (46%) | 48 (55%) | 6 (20%) | |
Unknown | 1 | 1 | 0 | |
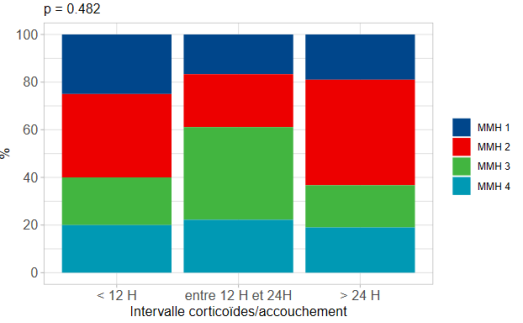
3.7. The Impact of the Interval Between the Last dose of Antenatal Corticosteroid Therapy and Delivery on the Severity of RDS (Figure 7)
Among those who were born less than 12 hours after the last dose of antenatal corticosteroid therapy, 40% had RDS grade 3 or 4. Similarly, among those born more than 24 hours after the last dose of antenatal corticosteroid therapy, 37% had an RDS grade 3 or 4. This difference was not statistically significant (p = 0.2).
Figure 7. The severity of RDS according to the interval between the last dose of antenatal corticosteroid therapy and delivery.
3.8. The Influence of the Cause of Prematurity on the Severity of RDS (Table 4)
The percentage of premature infants, who required ≥ 2 doses of surfactant following spontaneous prematurity, induced prematurity for fetal arrhythmia and induced prematurity for preeclampsia is 32%, 19% and 17% respectively. And the percentage of RDS grade 3 or 4 in these 3 groups is 45%, 44%, and 31% respectively. The number of surfactant doses received postnatally and the radiological severity of RDS were not significantly associated with the cause of prematurity (p-value 0.4 and 0.6 respectively).
Table 4. Influence of the Cause of Prematurity on the Severity of RDS.
| Cause de la prématurité | |
Characteristi | Total, N= 118 | Spontané, N = 66 | ARCF,= 16 | Prééclampsie N= 29 | autre, N = 7 | p-value |
Stade radio | | | | | | 0.6 |
MMH 1-2 | 70 (59%) | 36 (55%) | 9 (56%) | 20 (69%) | 5 (71%) | |
MMH 3-4 | 48 (41%) | 30 (45%) | 7 (44%) | 9 (31%) | 2 (29%) | |
nb.dose.curosurf | | | | | | 0.4 |
1 dose | 88 (75%) | 45 (68%) | 13 (81%) | 24 (83%) | 6 (86%) | |
≥2 doses | 30 (25%) | 21 (32%) | 3 (19%) | 5 (17%) | 1 (14%) | |
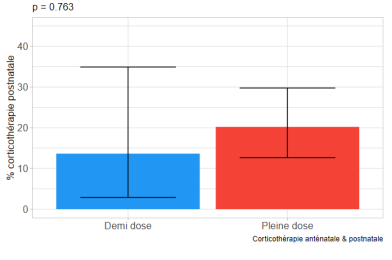
3.9. The Impact of the Number of Doses of Antenatal Corticosteroid Therapy on the Use of Postnatal Corticosteroid Therapy (Figure 8)
13% of patients who received 1 dose of antenatal corticosteroid therapy required postnatal corticosteroid therapy. Compared to 21% of patients who received 2 doses of antenatal corticosteroid therapy. The difference between the 2 groups is not statistically significant (p value 0.763).
Figure 8. Antenatal and Postnatal Corticosteroid Therapy.
3.10. The Impact of the Number of Doses of Antenatal Corticosteroid Therapy on the Complications of Prematurity (Table 5)
The durations of intubation and non-invasive ventilation were not statistically different between the 2 groups with respectively 1
| [1] | Simonetta Costa, Enrico Zecca, Daniele De Luca, Maria Pia De Carolis, Costantino Romagnoli. Efficacy of a single dose of antenatal corticosteroids on morbidity and mortality of preterm infants. Eur J Obstet Gynecol Reprod Biol. 2007 Apr; 131(2): 154-7. |
| [2] | Saliba E. Néonatalogie: bases scientifiques. 2017. (Elsevier Masson). |
| [3] | The American College of Obstetrics and Gynecology. Antenatal Corticosteroid Therapy for Fetal Maturation. Committee Opinion, Number 713, August 2017. |
| [4] | Xavier Miracle, Gian Carlo Di Renzo, Ann Stark, Avroy Fanaroff, Xavier Carbonell-Estrany, Erich Saling. Guideline for the use of antenatal corticosteroids for fetal maturation. J. Perinat. Med. 36(2008) 191–196. |
| [5] | Seger N, Soll R. Animal derived surfactant extract for treatment of respiratory distress syndrome. Cochrane Database Syst Rev. 2009; (2): CD007836. PMID: 19370695 https://doi.org/10.1002/14651858.CD007836 |
[1-5]
days and 4
| [2] | Saliba E. Néonatalogie: bases scientifiques. 2017. (Elsevier Masson). |
| [3] | The American College of Obstetrics and Gynecology. Antenatal Corticosteroid Therapy for Fetal Maturation. Committee Opinion, Number 713, August 2017. |
| [4] | Xavier Miracle, Gian Carlo Di Renzo, Ann Stark, Avroy Fanaroff, Xavier Carbonell-Estrany, Erich Saling. Guideline for the use of antenatal corticosteroids for fetal maturation. J. Perinat. Med. 36(2008) 191–196. |
| [5] | Seger N, Soll R. Animal derived surfactant extract for treatment of respiratory distress syndrome. Cochrane Database Syst Rev. 2009; (2): CD007836. PMID: 19370695 https://doi.org/10.1002/14651858.CD007836 |
| [6] | Sen S, Reghu A, Ferguson SD. Efficacy of a single dose of antenatal steroid in surfactant-treated babies under 31 weeks’ gestation. JMatern Fetal Neonatal Med 2002; 12: 298–303. PMID: 12607761 https://doi.org/10.1080/jmf.12.5.298.303 |
| [7] | Clamadieu C, Jarreau PH. Détresses respiratoires du nouveau-né́ (à l'exclusion de la pathologie ORL et Cardiaque), EMC 4-002-R-10; 1996. |
| [8] | Stéphanie Roberge, Yves Lacasse, SylvieTapp, YvesTremblay, Anneli Kari, Jing Liu, Myriam Fekih, Hussein S. Qublan, Melania M. Amorim, Emmanuel Bujold. Role of Fetal Sex in the Outcome of Antenatal Glucocorticoid Treatment to Prevent Respiratory Distress Syndrome: Systematic Review and Meta-Analysis. Journal of Obstetrics and Gynaecology Canada. Volume 33, Issue 3, March 2011, Pages 216-226. PMID: 21453561 https://doi.org/10.1016/s1701-2163(16)34822-8 |
| [9] | Suzanne L Miller, Mahalia Chai, Jan Loose, Margie Castillo-Meléndez, David W Walker, Graham Jenkin, Euan M Wallace. The effects of maternal betamethasone administration on the intrauterine growth-restricted fetus. Endocrinology 2007; 148(3): 1288–95. 27. PMID: 17158204 https://doi.org/10.1210/en.2006-1058 |
| [10] | Michal J Simchen, Fawaz Alkazaleh, S Lee Adamson, Rory Windrim, Joyce Telford, Joseph Beyene, John Kingdom. The fetal cardiovascular response to antenatal steroids in severe early-onset intrauterine growth restriction. Am J Obstet Gynecol 2004 Feb; 190(2): 296–304. PMID: 14981365 https://doi.org/10.1016/j.ajog.2003.08.011 |
| [11] | Andrew Elimian, Reinaldo Figueroa, Alan R Spitzer, Paul L Ogburn, Vandy Wiencek, J Gerald Quirk. Antenatal corticosteroids: are incomplete courses beneficial? Obstet Gynecol. 2003 Aug; 102(2): 352-5. PMID: 12907112 https://doi.org/10.1016/s0029-7844(03)00485-x |
| [12] | Chee-Ming Huang, Wu-Shiun Hsieh, Chien-Yi Chen, Po-Nien Tsao, Hung-Chieh Chou. Could Premature Infants Benefit from Single Dose Antenatal Betamethason. Research Gate. PMID: 23711674 https://doi.org/10.1016/j.pedneo.2013.04.005 |
| [13] | F. M. Regazzi, L. C. G. Silva, C. F. Lúcio, G. A. L. Veiga, D. S. R. Angrimani, C. I. Vannucchi. Morphometric and functional pulmonary changes of premature neonatal puppies after antenatal corticoid therapy. Theriogenology Volume 153, 1 September 2020, Pages 19-26 PMID: 32417607 https://doi.org/10.1016/j.theriogenology.2020.05.005 |
| [14] | D Roberts, S Dalziel. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst Rev. 2006 Jul 19; (3): CD004454. PMID: 33368142 PMCID: PMC8094626 https://doi.org/10.1002/14651858.CD004454.pub4 |
| [15] | T Lacaze-Masmonteil. Prenatal corticotherapy and acceleration of fetal maturation. Experimental and pharmacological data. Arch Pediatr. 1996 Nov; 3(11): 1111-7. PMID: 8952777 https://doi.org/10.1016/s0929-693x(96)89519-4 |
| [16] | Barbara J Stoll, Nellie I Hansen, Rosemary D Higgins, Eunice Kennedy Shriver. Neonatal outcomes of extremely preterm infants from the NICHD Neonatal Research Network. Pediatrics. 2010 Sep; 126(3): 443-56. PMID: 20732945 PMCID: PMC2982806 https://doi.org/10.1542/peds.2009-2959 |
| [17] | Alana J Westover, Timothy J M Moss. Effects of intrauterine infection or inflammation on fetal lung development. Clin Exp Pharmacol Physiol. 2012 Sep; 39(9): 824-30 PMID: 22816773 https://doi.org/10.1111/j.1440-1681.2012.05742.x |
| [18] | Committee on Fetus and Newborn; American Academy of Pediatrics. Respiratory support in preterm infants at birth. Pediatrics. 2014; 133(1): 171-174. |
| [19] | Walter-Nicolet E, Courtois E, Milesi C, et al. Premedication practices for delivery room intubations in premature infants in France: Results from the EPIPAGE 2 cohort study. PLoS One. 2019; 14(4): e0215150. https://doi.org/10.1371/journal.pone.0215150 |
| [20] | Pladys P, Berneau P, Beuchée A. Modalités non invasives d’instillation du surfactant exogène. /data/revues/0929693X/v22i5sS1/S0929693X15300518/ [Internet]. 2015 Jun 23; PMID: 26112542 https://doi.org/10.1016/S0929-693X(15)30051-8 |
| [21] | Sweet DG, Carnielli V, Greisen G, et al. European Consensus Guidelines on the Management of Respiratory Distress Syndrome - 2019 Update. Neonatology. 2019; 115(4): 432-450. PMID: 36863329 PMCID: PMC10064400 https://doi.org/10.1159/000528914 |
| [22] | Stevens TP, Harrington EW, Blennow M et al. Early surfactant administration with brief ventilation vs. selective surfactant and continued mechanical ventilation for preterm infants with or at risk for respiratory distress syndrome. Cochrane Database Syst Rev. 2007; (4): CD003063. PMID: 17943779 PMCID: PMC8554819 https://doi.org/10.1002/14651858.CD003063.pub3 |
| [23] | Kanmaz HG, Erdeve O, Canpolat FE et al. Surfactant administration via thin catheter during spontaneous breathing: randomized controlled trial. Pediatrics. 2013; 131(2): e502-e509. PMID: 23359581 https://doi.org/10.1542/peds.2012-0603 |
| [24] | Aldana-Aguirre JC, Pinto M, Featherstone RM et al. Less invasive surfactant administration versus intubation for surfactant delivery in preterm infants with respiratory distress syndrome: a systematic review and meta-analysis. Arch Dis Child Fetal Neonatal Ed. 2017; 102(1): F17-F23. PMID: 27852668 https://doi.org/10.1136/archdischild-2015-310299 |
| [25] | S J Stock, A J Thomson, S Papworth Antenatal Corticosteroids to Reduce Neonatal Morbidity and Mortality Green–top Guideline No. 7 October 2010. Royal College of Obstetricians and Gynaecologists. PMID: 35172391 https://doi.org/10.1111/1471-0528.17027 |
| [26] | M Kinalski, A Sledziewski, A Kretowski. Intrauterine stimulation for fetal respiratory system maturation; benefits and risks. Wiad Lek. 2000; 53(9-10): 538-45 PMID: 11148922. |
| [27] | D Roberts, S Dalziel. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst Rev 2006; (3): CD004454. PMID: 16856047 https://doi.org/10.1002/14651858.CD004454.pub2 |
| [28] | Natalia Saldaña-García, María Gracia Espinosa-Fernández, Celia Gómez-Robles et al. Benefits of a Single Dose of Betamethasone in Imminent Preterm Labour. J Clin Med. 2022 Jan; 11(1): 20. PMID: 35011761 PMCID: PMC8745219 https://doi.org/10.3390/jcm11010020 |
| [29] | David M Haas, William McCullough, Michael F McNamara, Cara Olsen. The first 48 hours: Comparing 12-hour and 24-hour betamethasone dosing when preterm deliveries occur rapidly. J Matern Fetal Neonatal Med. 2006 Jun; 19(6): 365-9. PMID: 16801314 https://doi.org/10.1080/14767050600715873 |
| [30] | Joonho Lee, Hyo Suk Seong. Evidence to support that spontaneous preterm labor is adaptive in nature: neonatal RDS is more common in "indicated" than in "spontaneous" preterm birth. J Perinat Med. 2009; 37(1): 53-8. PMID: 19099368 PMCID: PMC2887663 https://doi.org/10.1515/JPM.2009.036 |
| [31] | Fernanda Machado Regazzi, Beatriz Melo Justo. Prenatal or postnatal corticosteroids favor clinical, respiratory, metabolic outcomes and oxidative balance of preterm lambs corticotherapy for premature neonatal lambs. Theriogenology, Volume 182, 1 April 2022, Pages 129-137. PMID: 35168015 https://doi.org/10.1016/j.theriogenology.2022.02.006 |
| [32] | Tridente A, De Martino L, De Luca D. Porcine vs bovine surfactant therapy for preterm neonates with RDS: systematic review with biological plausibility and pragmatic meta-analysis of respiratory outcomes. Respir Res. 2019; 20(1): 28. PMID: 30728009 PMCID: PMC6366095 https://doi.org/10.1186/s12931-019-0979-0 |
| [33] | Lamboley-Gilmert G, Lacaze-Masmonteil T; Neonatologists of the Curosurf Postmarketing French Study. The short-term outcome of a large cohort of very preterm infants treated with poractant alfa (Curosurf) for respiratory distress syndrome. A postmarketing phase IV study. Paediatr Drugs. 2003; 5(9): 639-645. PMID: 12956620 https://doi.org/10.2165/00148581-200305090-00006 |
| [34] | O Baud, L Foix-L'Helias, M Kaminski et al. Antenatal glucocorticoid treatment and cystic periventricular leukomalacia in very premature infants. N Engl J Med. 1999 Oct 14; 341(16): 1190-6. PMID: 10519896 https://doi.org/10.1056/NEJM199910143411604 |
| [35] | W I Anyaegbunam, A B Adetona. Use of antenatal corticosteroids for fetal maturation in preterm infants. Am Fam Physician. 1997 Sep 15; 56(4): 1093-6 PMID: 9310061. |
[2-36]
days in group 1, and 2
| [1] | Simonetta Costa, Enrico Zecca, Daniele De Luca, Maria Pia De Carolis, Costantino Romagnoli. Efficacy of a single dose of antenatal corticosteroids on morbidity and mortality of preterm infants. Eur J Obstet Gynecol Reprod Biol. 2007 Apr; 131(2): 154-7. |
| [2] | Saliba E. Néonatalogie: bases scientifiques. 2017. (Elsevier Masson). |
| [3] | The American College of Obstetrics and Gynecology. Antenatal Corticosteroid Therapy for Fetal Maturation. Committee Opinion, Number 713, August 2017. |
| [4] | Xavier Miracle, Gian Carlo Di Renzo, Ann Stark, Avroy Fanaroff, Xavier Carbonell-Estrany, Erich Saling. Guideline for the use of antenatal corticosteroids for fetal maturation. J. Perinat. Med. 36(2008) 191–196. |
| [5] | Seger N, Soll R. Animal derived surfactant extract for treatment of respiratory distress syndrome. Cochrane Database Syst Rev. 2009; (2): CD007836. PMID: 19370695 https://doi.org/10.1002/14651858.CD007836 |
[1-5]
days respectively. And 13
| [3] | The American College of Obstetrics and Gynecology. Antenatal Corticosteroid Therapy for Fetal Maturation. Committee Opinion, Number 713, August 2017. |
| [4] | Xavier Miracle, Gian Carlo Di Renzo, Ann Stark, Avroy Fanaroff, Xavier Carbonell-Estrany, Erich Saling. Guideline for the use of antenatal corticosteroids for fetal maturation. J. Perinat. Med. 36(2008) 191–196. |
| [5] | Seger N, Soll R. Animal derived surfactant extract for treatment of respiratory distress syndrome. Cochrane Database Syst Rev. 2009; (2): CD007836. PMID: 19370695 https://doi.org/10.1002/14651858.CD007836 |
| [6] | Sen S, Reghu A, Ferguson SD. Efficacy of a single dose of antenatal steroid in surfactant-treated babies under 31 weeks’ gestation. JMatern Fetal Neonatal Med 2002; 12: 298–303. PMID: 12607761 https://doi.org/10.1080/jmf.12.5.298.303 |
| [7] | Clamadieu C, Jarreau PH. Détresses respiratoires du nouveau-né́ (à l'exclusion de la pathologie ORL et Cardiaque), EMC 4-002-R-10; 1996. |
| [8] | Stéphanie Roberge, Yves Lacasse, SylvieTapp, YvesTremblay, Anneli Kari, Jing Liu, Myriam Fekih, Hussein S. Qublan, Melania M. Amorim, Emmanuel Bujold. Role of Fetal Sex in the Outcome of Antenatal Glucocorticoid Treatment to Prevent Respiratory Distress Syndrome: Systematic Review and Meta-Analysis. Journal of Obstetrics and Gynaecology Canada. Volume 33, Issue 3, March 2011, Pages 216-226. PMID: 21453561 https://doi.org/10.1016/s1701-2163(16)34822-8 |
| [9] | Suzanne L Miller, Mahalia Chai, Jan Loose, Margie Castillo-Meléndez, David W Walker, Graham Jenkin, Euan M Wallace. The effects of maternal betamethasone administration on the intrauterine growth-restricted fetus. Endocrinology 2007; 148(3): 1288–95. 27. PMID: 17158204 https://doi.org/10.1210/en.2006-1058 |
| [10] | Michal J Simchen, Fawaz Alkazaleh, S Lee Adamson, Rory Windrim, Joyce Telford, Joseph Beyene, John Kingdom. The fetal cardiovascular response to antenatal steroids in severe early-onset intrauterine growth restriction. Am J Obstet Gynecol 2004 Feb; 190(2): 296–304. PMID: 14981365 https://doi.org/10.1016/j.ajog.2003.08.011 |
| [11] | Andrew Elimian, Reinaldo Figueroa, Alan R Spitzer, Paul L Ogburn, Vandy Wiencek, J Gerald Quirk. Antenatal corticosteroids: are incomplete courses beneficial? Obstet Gynecol. 2003 Aug; 102(2): 352-5. PMID: 12907112 https://doi.org/10.1016/s0029-7844(03)00485-x |
| [12] | Chee-Ming Huang, Wu-Shiun Hsieh, Chien-Yi Chen, Po-Nien Tsao, Hung-Chieh Chou. Could Premature Infants Benefit from Single Dose Antenatal Betamethason. Research Gate. PMID: 23711674 https://doi.org/10.1016/j.pedneo.2013.04.005 |
| [13] | F. M. Regazzi, L. C. G. Silva, C. F. Lúcio, G. A. L. Veiga, D. S. R. Angrimani, C. I. Vannucchi. Morphometric and functional pulmonary changes of premature neonatal puppies after antenatal corticoid therapy. Theriogenology Volume 153, 1 September 2020, Pages 19-26 PMID: 32417607 https://doi.org/10.1016/j.theriogenology.2020.05.005 |
| [14] | D Roberts, S Dalziel. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst Rev. 2006 Jul 19; (3): CD004454. PMID: 33368142 PMCID: PMC8094626 https://doi.org/10.1002/14651858.CD004454.pub4 |
| [15] | T Lacaze-Masmonteil. Prenatal corticotherapy and acceleration of fetal maturation. Experimental and pharmacological data. Arch Pediatr. 1996 Nov; 3(11): 1111-7. PMID: 8952777 https://doi.org/10.1016/s0929-693x(96)89519-4 |
| [16] | Barbara J Stoll, Nellie I Hansen, Rosemary D Higgins, Eunice Kennedy Shriver. Neonatal outcomes of extremely preterm infants from the NICHD Neonatal Research Network. Pediatrics. 2010 Sep; 126(3): 443-56. PMID: 20732945 PMCID: PMC2982806 https://doi.org/10.1542/peds.2009-2959 |
| [17] | Alana J Westover, Timothy J M Moss. Effects of intrauterine infection or inflammation on fetal lung development. Clin Exp Pharmacol Physiol. 2012 Sep; 39(9): 824-30 PMID: 22816773 https://doi.org/10.1111/j.1440-1681.2012.05742.x |
| [18] | Committee on Fetus and Newborn; American Academy of Pediatrics. Respiratory support in preterm infants at birth. Pediatrics. 2014; 133(1): 171-174. |
| [19] | Walter-Nicolet E, Courtois E, Milesi C, et al. Premedication practices for delivery room intubations in premature infants in France: Results from the EPIPAGE 2 cohort study. PLoS One. 2019; 14(4): e0215150. https://doi.org/10.1371/journal.pone.0215150 |
| [20] | Pladys P, Berneau P, Beuchée A. Modalités non invasives d’instillation du surfactant exogène. /data/revues/0929693X/v22i5sS1/S0929693X15300518/ [Internet]. 2015 Jun 23; PMID: 26112542 https://doi.org/10.1016/S0929-693X(15)30051-8 |
| [21] | Sweet DG, Carnielli V, Greisen G, et al. European Consensus Guidelines on the Management of Respiratory Distress Syndrome - 2019 Update. Neonatology. 2019; 115(4): 432-450. PMID: 36863329 PMCID: PMC10064400 https://doi.org/10.1159/000528914 |
| [22] | Stevens TP, Harrington EW, Blennow M et al. Early surfactant administration with brief ventilation vs. selective surfactant and continued mechanical ventilation for preterm infants with or at risk for respiratory distress syndrome. Cochrane Database Syst Rev. 2007; (4): CD003063. PMID: 17943779 PMCID: PMC8554819 https://doi.org/10.1002/14651858.CD003063.pub3 |
| [23] | Kanmaz HG, Erdeve O, Canpolat FE et al. Surfactant administration via thin catheter during spontaneous breathing: randomized controlled trial. Pediatrics. 2013; 131(2): e502-e509. PMID: 23359581 https://doi.org/10.1542/peds.2012-0603 |
| [24] | Aldana-Aguirre JC, Pinto M, Featherstone RM et al. Less invasive surfactant administration versus intubation for surfactant delivery in preterm infants with respiratory distress syndrome: a systematic review and meta-analysis. Arch Dis Child Fetal Neonatal Ed. 2017; 102(1): F17-F23. PMID: 27852668 https://doi.org/10.1136/archdischild-2015-310299 |
| [25] | S J Stock, A J Thomson, S Papworth Antenatal Corticosteroids to Reduce Neonatal Morbidity and Mortality Green–top Guideline No. 7 October 2010. Royal College of Obstetricians and Gynaecologists. PMID: 35172391 https://doi.org/10.1111/1471-0528.17027 |
| [26] | M Kinalski, A Sledziewski, A Kretowski. Intrauterine stimulation for fetal respiratory system maturation; benefits and risks. Wiad Lek. 2000; 53(9-10): 538-45 PMID: 11148922. |
| [27] | D Roberts, S Dalziel. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst Rev 2006; (3): CD004454. PMID: 16856047 https://doi.org/10.1002/14651858.CD004454.pub2 |
| [28] | Natalia Saldaña-García, María Gracia Espinosa-Fernández, Celia Gómez-Robles et al. Benefits of a Single Dose of Betamethasone in Imminent Preterm Labour. J Clin Med. 2022 Jan; 11(1): 20. PMID: 35011761 PMCID: PMC8745219 https://doi.org/10.3390/jcm11010020 |
| [29] | David M Haas, William McCullough, Michael F McNamara, Cara Olsen. The first 48 hours: Comparing 12-hour and 24-hour betamethasone dosing when preterm deliveries occur rapidly. J Matern Fetal Neonatal Med. 2006 Jun; 19(6): 365-9. PMID: 16801314 https://doi.org/10.1080/14767050600715873 |
| [30] | Joonho Lee, Hyo Suk Seong. Evidence to support that spontaneous preterm labor is adaptive in nature: neonatal RDS is more common in "indicated" than in "spontaneous" preterm birth. J Perinat Med. 2009; 37(1): 53-8. PMID: 19099368 PMCID: PMC2887663 https://doi.org/10.1515/JPM.2009.036 |
| [31] | Fernanda Machado Regazzi, Beatriz Melo Justo. Prenatal or postnatal corticosteroids favor clinical, respiratory, metabolic outcomes and oxidative balance of preterm lambs corticotherapy for premature neonatal lambs. Theriogenology, Volume 182, 1 April 2022, Pages 129-137. PMID: 35168015 https://doi.org/10.1016/j.theriogenology.2022.02.006 |
| [32] | Tridente A, De Martino L, De Luca D. Porcine vs bovine surfactant therapy for preterm neonates with RDS: systematic review with biological plausibility and pragmatic meta-analysis of respiratory outcomes. Respir Res. 2019; 20(1): 28. PMID: 30728009 PMCID: PMC6366095 https://doi.org/10.1186/s12931-019-0979-0 |
| [33] | Lamboley-Gilmert G, Lacaze-Masmonteil T; Neonatologists of the Curosurf Postmarketing French Study. The short-term outcome of a large cohort of very preterm infants treated with poractant alfa (Curosurf) for respiratory distress syndrome. A postmarketing phase IV study. Paediatr Drugs. 2003; 5(9): 639-645. PMID: 12956620 https://doi.org/10.2165/00148581-200305090-00006 |
| [34] | O Baud, L Foix-L'Helias, M Kaminski et al. Antenatal glucocorticoid treatment and cystic periventricular leukomalacia in very premature infants. N Engl J Med. 1999 Oct 14; 341(16): 1190-6. PMID: 10519896 https://doi.org/10.1056/NEJM199910143411604 |
| [35] | W I Anyaegbunam, A B Adetona. Use of antenatal corticosteroids for fetal maturation in preterm infants. Am Fam Physician. 1997 Sep 15; 56(4): 1093-6 PMID: 9310061. |
[3-39]
days in group 2 (p = 0.8 and 0.5 respectively).
In terms of complications, there were no statistically significant differences between the two groups. Indeed, 16% of patients in group 1 developed BPD compared to 17% in group 2 (p > 0.9). The risk of BPD was not significantly associated with either birth weight or gestational age (OR = 0.99 and 0.96; p = 0.2 and 0.8 respectively). The frequency of IVH, all grades combined, was 40% in group 1 and 33% in group 2 (p=0.3). The frequency of severe NEC was 0% in group 1 and 6.3% in group 2 (p= 0.6).
The mortality rate, from all causes, was 17% and 20% in groups 1 and 2 respectively (p > 0.9). In a multivariate analysis, the risk of death was associated within the limit of significance with gestational age (OR = 1.46; p = 0.001) with a reduction of 4% per additional week of gestation.
Table 5. Complications of prematurity according to the number of doses of antenatal corticosteroid therapy.
| Corticoïdes antenataux) | |
| Total, N= 118 | Demidose, N=23 | Pleinedose N=95 | p-value |
durée.d’intubation | 2.0 (1.0,5.0) | 1.0 (1.0,5.0) | 2.0 (1.0,5.0) | 0.8 |
durée.VNI | 12 (3, 39) | 4 (2, 36) | 13 (3, 39) | 0.5 |
pneumothorax | | | | 0.5 |
non | 115 (97%) | 22 (96%) | 93 (98%) | |
oui | 3 (2.5%) | 1 (4.3%) | 2 (2.1%) | |
Hémorragie pulmo | | | | 0.046 |
non | 111 (96%) | 19 (86%) | 92 (98%) | |
oui | 5 (4.3%) | 3 (14%) | 2 (2.1%) | |
DBP | | | | >0.9 |
non | 68 (83%) | 16 (84%) | 52 (83%) | |
oui | 14 (17%) | 3 (16%) | 11 (17%) | |
Unknown | 36 | 4 | 32 | |
HIV | | | | 0.3 |
non | 73 (66%) | 12 (60%) | 61 (67%) | |
grade 1 | 11 (9.9%) | 1 (5.0%) | 10 (11%) | |
grade 2 | 14 (13%) | 2 (10%) | 12 (13%) | |
grade 3 | 5 (4.5%) | 2 (10%) | 3 (3.3%) | |
grade 4 | 8 (7.2%) | 3 (15%) | 5 (5.5%) | |
Unknown | 7 | 3 | 4 | |
durée.hopital | 45 (11,67) | 38 (18, 77) | 45 (11, 65) | 0.7 |
ECUN.sévère | | | | 0.6 |
non | 112 (95%) | 23 (100%) | 89 (94%) | |
oui | 6 (5.1%) | 0 (0%) | 6 (6.3%) | |
Décès | | | | >0.9 |
oui | 23 (19%) | 4 (17%) | 19 (20%) | |
Non (Vivant) | 95 (81%) | 19 (83%) | 76 (80%) | |
4. Discussion
The main objective of our study is to evaluate the effectiveness of a complete versus incomplete course of antenatal corticosteroid therapy, on the number of doses of surfactant received postnatally in a premature infant with RDS, by comparing two groups: group 1 (1 dose of antenatal corticosteroid therapy) and group 2 (2 doses of antenatal corticosteroid therapy).
The clinical characteristics of the newborns were comparable in the two groups (sex ratio, gestational age and birth weight).
Roberge et al showed that the effect of antenatal corticosteroid therapy on the prevention of RDS is similar in male and female newborns
| [8] | Stéphanie Roberge, Yves Lacasse, SylvieTapp, YvesTremblay, Anneli Kari, Jing Liu, Myriam Fekih, Hussein S. Qublan, Melania M. Amorim, Emmanuel Bujold. Role of Fetal Sex in the Outcome of Antenatal Glucocorticoid Treatment to Prevent Respiratory Distress Syndrome: Systematic Review and Meta-Analysis. Journal of Obstetrics and Gynaecology Canada. Volume 33, Issue 3, March 2011, Pages 216-226. PMID: 21453561 https://doi.org/10.1016/s1701-2163(16)34822-8 |
[8]
.
There was no statistically significant difference between the two groups regarding IUGR. Miller et al
| [9] | Suzanne L Miller, Mahalia Chai, Jan Loose, Margie Castillo-Meléndez, David W Walker, Graham Jenkin, Euan M Wallace. The effects of maternal betamethasone administration on the intrauterine growth-restricted fetus. Endocrinology 2007; 148(3): 1288–95. 27. PMID: 17158204 https://doi.org/10.1210/en.2006-1058 |
[9]
showed that IUGR fetuses exposed to betamethasone have a disturbance in cerebral blood flow which is not observed in healthy fetuses, this contributes to an increased incidence of cell death. This invite us to consider the indications for antenatal corticosteroid therapy in premature infants with IUGR
| [10] | Michal J Simchen, Fawaz Alkazaleh, S Lee Adamson, Rory Windrim, Joyce Telford, Joseph Beyene, John Kingdom. The fetal cardiovascular response to antenatal steroids in severe early-onset intrauterine growth restriction. Am J Obstet Gynecol 2004 Feb; 190(2): 296–304. PMID: 14981365 https://doi.org/10.1016/j.ajog.2003.08.011 |
[10]
.
The main criterion in our study is the number of doses of surfactant received postnatally (1 dose or ≥ 2 doses) depending on the number of doses of antenatal corticosteroid therapy (group 1 versus group 2). We did not find any statistically significant difference between the two groups regarding this criterion.
The percentage of premature infants who received ≥ 2 doses of surfactant is 30% and 25% for group 1 and 2 respectively, with a p value 0.596, OR 0.73 and IC 95%, 0.25 to 2.37. This shows that just like a complete course, an incomplete course of antenatal corticosteroid therapy can also act on the severity of RDS.
On the other hand, unlike a complete course of antenatal corticosteroid therapy, there are very few studies concerning the advantages of an incomplete course.
Costa et al
| [1] | Simonetta Costa, Enrico Zecca, Daniele De Luca, Maria Pia De Carolis, Costantino Romagnoli. Efficacy of a single dose of antenatal corticosteroids on morbidity and mortality of preterm infants. Eur J Obstet Gynecol Reprod Biol. 2007 Apr; 131(2): 154-7. |
[1]
, in a retrospective cohort study including 411 premature babies between 25 and 34 weeks divided into two groups; Group 1 of 170 newborns exposed before delivery to a single dose of 12 mg of betamethasone and group 2 of 241 newborns who did not receive antenatal corticosteroid therapy; compared the results according to gestational age subclasses. They found in the subgroup of 25 to 27 weeks that intubation in the delivery room, surfactant treatment and PDA were less frequent in the newborns of group 1 with also shorter duration of ventilation and oxygen therapy. These results are comparable to those of the subgroup 30 to 31 weeks. On the other hand, no difference was found in the 28-29 weeks subgroup and in the 32-34 weeks subgroup. Finally, they concluded that the effects of an incomplete course of antenatal corticosteroid therapy depend on the gestational age subgroups. Similarly, Elimian et al
| [11] | Andrew Elimian, Reinaldo Figueroa, Alan R Spitzer, Paul L Ogburn, Vandy Wiencek, J Gerald Quirk. Antenatal corticosteroids: are incomplete courses beneficial? Obstet Gynecol. 2003 Aug; 102(2): 352-5. PMID: 12907112 https://doi.org/10.1016/s0029-7844(03)00485-x |
[11]
, in a retrospective study including 229 premature babies between 23 and 34 weeks, divided into two groups; Group 1 of 125 newborns exposed to a dose of 12 mg of dexamethasone and group 2 of 104 newborns who did not receive antenatal corticosteroid therapy; concluded that an incomplete course of antenatal corticosteroid therapy is associated with a reduction in the need for vasopressors, the rate of IVH and neonatal mortality in premature newborns. Similarly, Huang et al
| [12] | Chee-Ming Huang, Wu-Shiun Hsieh, Chien-Yi Chen, Po-Nien Tsao, Hung-Chieh Chou. Could Premature Infants Benefit from Single Dose Antenatal Betamethason. Research Gate. PMID: 23711674 https://doi.org/10.1016/j.pedneo.2013.04.005 |
[12]
showed that a single dose of antenatal corticosteroid therapy can reduce the need for surfactants and vasopressors in premature babies between 24 and 34 weeks. This justify that obstetricians should not hesitate to prescribe antenatal corticosteroids even if a complete course is not feasible.
In our study, the antenatal corticosteroid therapy used was betamethasone. It is the drug of choice for artificially improving lung function. Regazzi et al
| [13] | F. M. Regazzi, L. C. G. Silva, C. F. Lúcio, G. A. L. Veiga, D. S. R. Angrimani, C. I. Vannucchi. Morphometric and functional pulmonary changes of premature neonatal puppies after antenatal corticoid therapy. Theriogenology Volume 153, 1 September 2020, Pages 19-26 PMID: 32417607 https://doi.org/10.1016/j.theriogenology.2020.05.005 |
[13]
tried to understand the effect of antenatal corticosteroid therapy on the lung development of premature puppies. They concluded that it acts on the development of gas exchange zones in the lungs, rather than by stimulating the production of surfactant. Antenatal corticosteroid therapy accelerates lung maturation by enhancing the production of type I pneumocytes, which increase lung volume and compliance, and type II pneumocytes, which produce surfactant and reduce tension in the alveoli, to help prevent atelectasis and optimize gas exchange
| [14] | D Roberts, S Dalziel. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst Rev. 2006 Jul 19; (3): CD004454. PMID: 33368142 PMCID: PMC8094626 https://doi.org/10.1002/14651858.CD004454.pub4 |
[14]
.
Betamethasone is a fluorinated corticosteroid that has weak mineralocorticoid activity. After a single treatment, it does not inhibit the adrenal response to postnatal stress; however, repeated courses can induce adrenal depression if a stressful event occurs after birth
.
By looking for other factors that could influence the number of doses of surfactant received, we found that the term, the presence of an infection, and the severity in the delivery room (intubation, resuscitation, etc.) seem to influence the number of doses of surfactant received. We will compare the influence of each of these factors compared to the literature.
The study about the influence of the term on the number of doses of surfactants shows that the percentage of premature babies who needed ≥ 2 doses of surfactant between 32 and 37 weeks, between 28 and 32 weeks and in very premature babies < 28 SA is 33%, 14% and 39% respectively with a statistically significant difference between the 3 groups (p < 0.001). Our results are not correlated with the data available in the literature which show that the radiological severity of RDS is inversely proportional to gestational age
| [16] | Barbara J Stoll, Nellie I Hansen, Rosemary D Higgins, Eunice Kennedy Shriver. Neonatal outcomes of extremely preterm infants from the NICHD Neonatal Research Network. Pediatrics. 2010 Sep; 126(3): 443-56. PMID: 20732945 PMCID: PMC2982806 https://doi.org/10.1542/peds.2009-2959 |
[16]
. This may be due to the fact that we tend to intervene less early on RDS in premature babies between 32 and 37 weeks, and that we only intervene for very severe RDS, which explains why they immediately need more doses of surfactant. We add that the indications for surfactant treatment in our department depend on the radiological grade of the RDS and the clinical severity. Knowing that this grade is defined by the neonatologist on call, who is not always the same, and not by the radiologist; this may create bias in our study.
Our study shows that neonatal sepsis increases the severity of RDS, which is not correlated with literature data. We found that 58% of preterm infants with confirmed neonatal sepsis required ≥2 doses of surfactants. Compared to 17% of premature babies without risk of neonatal sepsis (p=0.012). This can be explained by the fact that during data collection we considered as confirmed neonatal sepsis all those who had a positive blood culture but also probable neonatal sepsis who had negative blood cultures and had received ≥ 7 days of antibiotics. Westover et al showed that experimentally induced intrauterine infection in sheep causes an early increase in surfactant in premature lungs improving lung function and compliance, consistent with a reduced risk of RDS in human infants exposed to infection before birth
.
We observed in our study that premature babies in the delivery room who were intubated with or without drug administration required more doses of surfactant. Some were intubated severe RDS at birth, and others were intubated for other reasons. In the delivery room, the American Academy of Pediatrics
| [18] | Committee on Fetus and Newborn; American Academy of Pediatrics. Respiratory support in preterm infants at birth. Pediatrics. 2014; 133(1): 171-174. |
[18]
recommends the use of early non-invasive ventilation such as CPAP immediately after birth in premature infants, with secondary administration of exogenous surfactant if necessary (level of evidence 1). If mechanical ventilation is essential, extubation should be performed as soon as possible in order to reduce morbidity and mortality
| [18] | Committee on Fetus and Newborn; American Academy of Pediatrics. Respiratory support in preterm infants at birth. Pediatrics. 2014; 133(1): 171-174. |
[18]
. In our cohort, we did an immediate intubation in the delivery room in 11 cases (48%) in group 1 compared to 48 cases (51%) in group 2. This remains high compared to the data collected in EPIPAGE 2 with an incidence of 37%
| [19] | Walter-Nicolet E, Courtois E, Milesi C, et al. Premedication practices for delivery room intubations in premature infants in France: Results from the EPIPAGE 2 cohort study. PLoS One. 2019; 14(4): e0215150. https://doi.org/10.1371/journal.pone.0215150 |
[19]
. In our cohort, the risk of intubation in the delivery room was significantly associated with gestational age (OR = 0.88; p < 0.001) with a reduction in the risk of intubation of 12% per additional week of gestation.
Surfactant admministration was done by tracheal intubation in more than 95% of cases in our 2 groups. This technique is invasive, new methods of administering of exogenous surfactant have emerged
| [20] | Pladys P, Berneau P, Beuchée A. Modalités non invasives d’instillation du surfactant exogène. /data/revues/0929693X/v22i5sS1/S0929693X15300518/ [Internet]. 2015 Jun 23; PMID: 26112542 https://doi.org/10.1016/S0929-693X(15)30051-8 |
[20]
. The “InSurE” method which reduces the use of mechanical ventilation
| [21] | Sweet DG, Carnielli V, Greisen G, et al. European Consensus Guidelines on the Management of Respiratory Distress Syndrome - 2019 Update. Neonatology. 2019; 115(4): 432-450. PMID: 36863329 PMCID: PMC10064400 https://doi.org/10.1159/000528914 |
| [22] | Stevens TP, Harrington EW, Blennow M et al. Early surfactant administration with brief ventilation vs. selective surfactant and continued mechanical ventilation for preterm infants with or at risk for respiratory distress syndrome. Cochrane Database Syst Rev. 2007; (4): CD003063. PMID: 17943779 PMCID: PMC8554819 https://doi.org/10.1002/14651858.CD003063.pub3 |
[21, 22]
, and the minimally invasive “LISA” method which reduces the duration of mechanical ventilation, the incidence of BPD and death compared to the method “InSurE”
| [23] | Kanmaz HG, Erdeve O, Canpolat FE et al. Surfactant administration via thin catheter during spontaneous breathing: randomized controlled trial. Pediatrics. 2013; 131(2): e502-e509. PMID: 23359581 https://doi.org/10.1542/peds.2012-0603 |
| [24] | Aldana-Aguirre JC, Pinto M, Featherstone RM et al. Less invasive surfactant administration versus intubation for surfactant delivery in preterm infants with respiratory distress syndrome: a systematic review and meta-analysis. Arch Dis Child Fetal Neonatal Ed. 2017; 102(1): F17-F23. PMID: 27852668 https://doi.org/10.1136/archdischild-2015-310299 |
[23, 24]
. In our department, InSurE and LISA were still very little practiced at the time of the study. Indeed, only 1 and 2 patients in group 1, and 2 and 3 patients in group 2 were able to benefit from the LISA and InSurE method respectively. This is due to the fact that intubations and invasive procedures are not performed without sedation in our department, this is why the child often remains under the effect of sedation after InSurE, making early extubation difficult. The LISA method was started in our department in May 2019 and is now increasingly practiced since the introduction of a Ketamine sedation protocol.
We did not find a statistically significant difference in the radiological grade of RDS depending on the time between the last dose of antenatal corticosteroid therapy and delivery. Antenatal corticosteroids are most effective in reducing the risk of RDS in pregnancies that deliver 24 hours and up to 7 days after administration of the second dose of antenatal corticosteroids
| [25] | S J Stock, A J Thomson, S Papworth Antenatal Corticosteroids to Reduce Neonatal Morbidity and Mortality Green–top Guideline No. 7 October 2010. Royal College of Obstetricians and Gynaecologists. PMID: 35172391 https://doi.org/10.1111/1471-0528.17027 |
[25]
. On the other hand, Kinalski et al
| [26] | M Kinalski, A Sledziewski, A Kretowski. Intrauterine stimulation for fetal respiratory system maturation; benefits and risks. Wiad Lek. 2000; 53(9-10): 538-45 PMID: 11148922. |
[26]
showed that treatment lasting less than 24 hours can also improve results, which is comparable to what was found in our study. Among those born less than 12 hours after the last dose of antenatal corticosteroid therapy, 40% developed RDS grade 3-4 compared to 37% of those born more than 24 hours after the last dose of antenatal corticosteroid therapy, and the difference is not statistically significant, with a p value of 0.2. Roberts et al
| [27] | D Roberts, S Dalziel. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst Rev 2006; (3): CD004454. PMID: 16856047 https://doi.org/10.1002/14651858.CD004454.pub2 |
[27]
showed that antenatal corticosteroid therapy reduces neonatal mortality even when infants are born less than 24 hours after administration of the first dose (RR 0.53, 95% CI 0.29-0.96, four studies, 295 infants). Saldaña-García et al
| [28] | Natalia Saldaña-García, María Gracia Espinosa-Fernández, Celia Gómez-Robles et al. Benefits of a Single Dose of Betamethasone in Imminent Preterm Labour. J Clin Med. 2022 Jan; 11(1): 20. PMID: 35011761 PMCID: PMC8745219 https://doi.org/10.3390/jcm11010020 |
[28]
showed that a single dose of betamethasone up to 3 hours before delivery can reduce the severity of RDS as well as other severe complications of prematurity, especially in non-tertiary hospitals. Regarding the interval between the two doses of betamethasone, M Haas et al
| [29] | David M Haas, William McCullough, Michael F McNamara, Cara Olsen. The first 48 hours: Comparing 12-hour and 24-hour betamethasone dosing when preterm deliveries occur rapidly. J Matern Fetal Neonatal Med. 2006 Jun; 19(6): 365-9. PMID: 16801314 https://doi.org/10.1080/14767050600715873 |
[29]
concluded that administering betamethasone at 12-hour intervals can result in similar neonatal outcomes compared to the standard 24-hour regimen, When the delivery occurs within 48 hours after starting the treatment.
In our study, we observed that the cause of prematurity does not influence the severity of RDS. Whether spontaneous or induced delivery for preeclampsia or fetal arrythmia or other, there is no effect on the radiological grade of RDS, nor the number of surfactant doses received postnatally. Lee et al
| [30] | Joonho Lee, Hyo Suk Seong. Evidence to support that spontaneous preterm labor is adaptive in nature: neonatal RDS is more common in "indicated" than in "spontaneous" preterm birth. J Perinat Med. 2009; 37(1): 53-8. PMID: 19099368 PMCID: PMC2887663 https://doi.org/10.1515/JPM.2009.036 |
[30]
conducted a retrospective study including 257 premature babies between 24 and 32 weeks, divided into two groups according to the etiology of premature birth. Group 1 spontaneous prematurity and group 2 induced prematurity. They concluded that the RDS level is higher after induced prematurity; This finding supports the idea that spontaneous preterm labor is adaptive in nature.
Postnatal corticosteroid therapy was used in 16% of patients in group 1 compared to 17% of patients in group 2. The molecule used was betamethasone with a short course of 3 days with the aim of successful extubation and/or to reduce the severity of a BPD. No statistically significant difference between the two groups (p= 0.763). We concluded that the number of doses of antenatal corticosteroid therapy does not influence the use of postnatal corticosteroids.
Antenatal corticosteroid therapy induces structural and functional lung maturation, while postnatal corticosteroid therapy treats lung inflammation and support lung development
| [31] | Fernanda Machado Regazzi, Beatriz Melo Justo. Prenatal or postnatal corticosteroids favor clinical, respiratory, metabolic outcomes and oxidative balance of preterm lambs corticotherapy for premature neonatal lambs. Theriogenology, Volume 182, 1 April 2022, Pages 129-137. PMID: 35168015 https://doi.org/10.1016/j.theriogenology.2022.02.006 |
[31]
. Therefore, antenatal and postnatal corticosteroid therapy have been proposed for many years as interventions to prevent RDS and BPD in premature newborns, respectively
| [31] | Fernanda Machado Regazzi, Beatriz Melo Justo. Prenatal or postnatal corticosteroids favor clinical, respiratory, metabolic outcomes and oxidative balance of preterm lambs corticotherapy for premature neonatal lambs. Theriogenology, Volume 182, 1 April 2022, Pages 129-137. PMID: 35168015 https://doi.org/10.1016/j.theriogenology.2022.02.006 |
[31]
. There is little literature regarding the influence of the number of doses of antenatal corticosteroid therapy on postnatal corticosteroid therapy.
The use of postnatal corticosteroid therapy remains controversial. Dexamethasone reduces the risk of BPD and increases the chances of extubation but at the expense of an increased risk of neurological sequelae such as cerebral palsy, especially if it is used during the first week
| [21] | Sweet DG, Carnielli V, Greisen G, et al. European Consensus Guidelines on the Management of Respiratory Distress Syndrome - 2019 Update. Neonatology. 2019; 115(4): 432-450. PMID: 36863329 PMCID: PMC10064400 https://doi.org/10.1159/000528914 |
[21]
. In 2019, the European Consensus Guidelines on the Management of Respiratory Distress Syndrome recommends the administration of low dose dexamethasone to facilitate extubation in newborns who require conventional ventilation after 1 to 2 weeks (grade A2 recommendation)
| [21] | Sweet DG, Carnielli V, Greisen G, et al. European Consensus Guidelines on the Management of Respiratory Distress Syndrome - 2019 Update. Neonatology. 2019; 115(4): 432-450. PMID: 36863329 PMCID: PMC10064400 https://doi.org/10.1159/000528914 |
[21]
.
In our population, 16% of patients in group 1 developed BPD compared to 17% in group 2 (p > 0.9). The risk of occurrence of BPD was not significantly associated with the number of doses of antenatal corticosteroid therapy. There are very few studies concerning the influence of the number of doses of antenatal corticosteroid therapy on the occurrence of BPD. The risk of BPD was not significantly associated with either birth weight or gestational age (OR = 0.99 and 0.98 e; p = 0.29 and 0.64 respectively), on the other hand literature data shows that BPD is inversely proportional to term
| [32] | Tridente A, De Martino L, De Luca D. Porcine vs bovine surfactant therapy for preterm neonates with RDS: systematic review with biological plausibility and pragmatic meta-analysis of respiratory outcomes. Respir Res. 2019; 20(1): 28. PMID: 30728009 PMCID: PMC6366095 https://doi.org/10.1186/s12931-019-0979-0 |
[32]
, but perhaps the number was insufficient to demonstrate it. Similarly, Lamboley-Gilmert G et al
| [33] | Lamboley-Gilmert G, Lacaze-Masmonteil T; Neonatologists of the Curosurf Postmarketing French Study. The short-term outcome of a large cohort of very preterm infants treated with poractant alfa (Curosurf) for respiratory distress syndrome. A postmarketing phase IV study. Paediatr Drugs. 2003; 5(9): 639-645. PMID: 12956620 https://doi.org/10.2165/00148581-200305090-00006 |
[33]
found that the risk factors for BPD were: small gestational age, low birth weight, poor response to the first dose of surfactant, the presence of pneumothorax or pulmonary hemorrhage and persistence ductus arteriosus.
The mortality rate was 17% and 20% in groups 1 and 2, respectively (p=0.9). In a multivariate analysis, the risk of death is significantly with gestational age (OR=0.95; p=0.05) with a reduction of 4% per additional week of gestation independently of the number of doses of antenatal corticosteroid therapy (OR=0.99; p=0.98). It was also associated with the occurrence of BPD (OR=0.74; p=0.0008) independently of the number of doses of antenatal corticosteroid therapy (OR=1.042; p=0.54).
We also found that the durations of intubation and non-invasive ventilation were not statistically different between the 2 groups (p = 0.8 and 0.5 respectively).
In terms of complications specific to prematurity, IVH was noted in 40% in group 1 and 33% in group 2 (p = 0.3). These results are comparable to those of EPIPAGE 2 with an incidence of 36% for all stages combined. In our patients, the severity of IVH was not significantly associated with the number of doses of antenatal corticosteroid therapy (p = 0.286). We observed more IVH grade 3-4 in group 1 than in group 2, but the difference is not statistically significant. Baud et al
| [34] | O Baud, L Foix-L'Helias, M Kaminski et al. Antenatal glucocorticoid treatment and cystic periventricular leukomalacia in very premature infants. N Engl J Med. 1999 Oct 14; 341(16): 1190-6. PMID: 10519896 https://doi.org/10.1056/NEJM199910143411604 |
[34]
conducted a study of 883 premature babies between 24 and 31 weeks, divided into 3 groups. Group 1 received a course of betamethasone before delivery, group 2 received a course of dexamethasone before delivery and group 3 did not receive antenatal corticosteroid therapy. They concluded that antenatal exposure to betamethasone but not dexamethasone is associated with a reduced risk of cystic periventricular leukomalacia in very premature newborns.
Severe NEC was noted in 0% in group 1 and 6.3% in group 2 (p=0.6). No statistically significant difference between the two groups.
Antenatal corticosteroid therapy is associated with a significant reduction in neonatal mortality, RDS and IVH rates
| [14] | D Roberts, S Dalziel. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst Rev. 2006 Jul 19; (3): CD004454. PMID: 33368142 PMCID: PMC8094626 https://doi.org/10.1002/14651858.CD004454.pub4 |
[14]
. A Cochrane review of 21 studies (3885 women and 4269 infants) showed that treating women at risk of preterm birth with a single course of antenatal corticosteroids reduced the risk of mortality by 31% (95% CI 19-42 %), RDS 44% (95% CI 31-57%) and IVH 46% (95% CI 31% to 67%)
| [14] | D Roberts, S Dalziel. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst Rev. 2006 Jul 19; (3): CD004454. PMID: 33368142 PMCID: PMC8094626 https://doi.org/10.1002/14651858.CD004454.pub4 |
[14]
. Antenatal corticosteroid therapy is also associated with a reduction in necrotizing enterocolitis, respiratory support, intensive care admissions, and systemic infections in the first 48 hours of life compared with no treatment or placebo treatment.
| [14] | D Roberts, S Dalziel. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst Rev. 2006 Jul 19; (3): CD004454. PMID: 33368142 PMCID: PMC8094626 https://doi.org/10.1002/14651858.CD004454.pub4 |
[14]
.
W I Anyaegbunam et al
| [35] | W I Anyaegbunam, A B Adetona. Use of antenatal corticosteroids for fetal maturation in preterm infants. Am Fam Physician. 1997 Sep 15; 56(4): 1093-6 PMID: 9310061. |
[35]
showed that corticosteroids are used in less than 20% of eligible patients. This trend will likely be considered as an unacceptable deviation from the standards of appropriate care. Antenatal counseling programs should educate pregnant women on the early recognition of conditions that may lead to premature birth. This approach would ensure early presentation and initiation of treatment.
M Kinalski et al
| [26] | M Kinalski, A Sledziewski, A Kretowski. Intrauterine stimulation for fetal respiratory system maturation; benefits and risks. Wiad Lek. 2000; 53(9-10): 538-45 PMID: 11148922. |
[26]
showed that the benefits derived from antenatal corticosteroid therapy is added to those of postnatal surfactant, making the latter more effective.
5. Conclusion
A complete course of antenatal corticosteroid therapy is recommended between 24 weeks and 34 weeks; it reduces the risk of developing RDS in premature babies. However, there are very few studies concerning the advantages of an incomplete course of antenatal corticosteroid therapy, hence the interest in carrying out this study to evaluate the effectiveness of a complete versus incomplete course of antenatal corticosteroid therapy, on the number of doses of surfactant received postnatally in a premature baby with hyaline membrane disease.
The number of doses of surfactant received postnatally is influenced by the term of birth, the presence of an neonatal sepsis and by resuscitation in the delivery room. The severity of RDS is not influenced either by the interval between the last dose of antenatal corticosteroid therapy or by the cause of prematurity.
Our study does not seem to show a statistically significant difference between 1 and 2 doses of antenatal corticosteroid therapy, in terms of clinical and radiological severity of RDS and in terms of the number of doses of surfactant necessary.
Likewise, no statistically significant difference was demonstrated in clinical improvement (duration of intubation, duration of non-invasive ventilation), in the need for postnatal corticosteroid therapy and in the risk of occurrence of morbidity and mortality (mortality rate, occurrence of BPD, IVH, severe NEC) between two groups of patients who received 1 dose or two doses of antenatal corticosteroid therapy.
However, other prospective randomized studies should be considered for a formal determination of the neonatal effects of a complete versus incomplete course of antenatal corticosteroid therapy, including BETADOSE, a double-blind, multicenter, randomized controlled trial testing the hypothesis that an imcomplete course of antenatal betamethasone is non-inferior to treatment with the full dose.
Abbreviations
GA: Gestational Age
RDS: Respiratory Distress Syndrome
BPD: Bronchopulmonary Dysplasia
PDA: Patent Ductus Arteriosus
LISA: Less Invasive Surfactant Administration
CPAP: Continuous Positive Airway Pressure
InSurE: Intubation, Surfactant Administration, Extubation
NEC: Necrotizing Enterocolitis
IVH: Intraventricular Hemorrhage
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Simonetta Costa, Enrico Zecca, Daniele De Luca, Maria Pia De Carolis, Costantino Romagnoli. Efficacy of a single dose of antenatal corticosteroids on morbidity and mortality of preterm infants. Eur J Obstet Gynecol Reprod Biol. 2007 Apr; 131(2): 154-7.
|
| [2] |
Saliba E. Néonatalogie: bases scientifiques. 2017. (Elsevier Masson).
|
| [3] |
The American College of Obstetrics and Gynecology. Antenatal Corticosteroid Therapy for Fetal Maturation. Committee Opinion, Number 713, August 2017.
|
| [4] |
Xavier Miracle, Gian Carlo Di Renzo, Ann Stark, Avroy Fanaroff, Xavier Carbonell-Estrany, Erich Saling. Guideline for the use of antenatal corticosteroids for fetal maturation. J. Perinat. Med. 36(2008) 191–196.
|
| [5] |
Seger N, Soll R. Animal derived surfactant extract for treatment of respiratory distress syndrome. Cochrane Database Syst Rev. 2009; (2): CD007836. PMID: 19370695
https://doi.org/10.1002/14651858.CD007836
|
| [6] |
Sen S, Reghu A, Ferguson SD. Efficacy of a single dose of antenatal steroid in surfactant-treated babies under 31 weeks’ gestation. JMatern Fetal Neonatal Med 2002; 12: 298–303. PMID: 12607761
https://doi.org/10.1080/jmf.12.5.298.303
|
| [7] |
Clamadieu C, Jarreau PH. Détresses respiratoires du nouveau-né́ (à l'exclusion de la pathologie ORL et Cardiaque), EMC 4-002-R-10; 1996.
|
| [8] |
Stéphanie Roberge, Yves Lacasse, SylvieTapp, YvesTremblay, Anneli Kari, Jing Liu, Myriam Fekih, Hussein S. Qublan, Melania M. Amorim, Emmanuel Bujold. Role of Fetal Sex in the Outcome of Antenatal Glucocorticoid Treatment to Prevent Respiratory Distress Syndrome: Systematic Review and Meta-Analysis. Journal of Obstetrics and Gynaecology Canada. Volume 33, Issue 3, March 2011, Pages 216-226. PMID: 21453561
https://doi.org/10.1016/s1701-2163(16)34822-8
|
| [9] |
Suzanne L Miller, Mahalia Chai, Jan Loose, Margie Castillo-Meléndez, David W Walker, Graham Jenkin, Euan M Wallace. The effects of maternal betamethasone administration on the intrauterine growth-restricted fetus. Endocrinology 2007; 148(3): 1288–95. 27. PMID: 17158204
https://doi.org/10.1210/en.2006-1058
|
| [10] |
Michal J Simchen, Fawaz Alkazaleh, S Lee Adamson, Rory Windrim, Joyce Telford, Joseph Beyene, John Kingdom. The fetal cardiovascular response to antenatal steroids in severe early-onset intrauterine growth restriction. Am J Obstet Gynecol 2004 Feb; 190(2): 296–304. PMID: 14981365
https://doi.org/10.1016/j.ajog.2003.08.011
|
| [11] |
Andrew Elimian, Reinaldo Figueroa, Alan R Spitzer, Paul L Ogburn, Vandy Wiencek, J Gerald Quirk. Antenatal corticosteroids: are incomplete courses beneficial? Obstet Gynecol. 2003 Aug; 102(2): 352-5. PMID: 12907112
https://doi.org/10.1016/s0029-7844(03)00485-x
|
| [12] |
Chee-Ming Huang, Wu-Shiun Hsieh, Chien-Yi Chen, Po-Nien Tsao, Hung-Chieh Chou. Could Premature Infants Benefit from Single Dose Antenatal Betamethason. Research Gate. PMID: 23711674
https://doi.org/10.1016/j.pedneo.2013.04.005
|
| [13] |
F. M. Regazzi, L. C. G. Silva, C. F. Lúcio, G. A. L. Veiga, D. S. R. Angrimani, C. I. Vannucchi. Morphometric and functional pulmonary changes of premature neonatal puppies after antenatal corticoid therapy. Theriogenology Volume 153, 1 September 2020, Pages 19-26 PMID: 32417607
https://doi.org/10.1016/j.theriogenology.2020.05.005
|
| [14] |
D Roberts, S Dalziel. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst Rev. 2006 Jul 19; (3): CD004454. PMID: 33368142 PMCID: PMC8094626
https://doi.org/10.1002/14651858.CD004454.pub4
|
| [15] |
T Lacaze-Masmonteil. Prenatal corticotherapy and acceleration of fetal maturation. Experimental and pharmacological data. Arch Pediatr. 1996 Nov; 3(11): 1111-7. PMID: 8952777
https://doi.org/10.1016/s0929-693x(96)89519-4
|
| [16] |
Barbara J Stoll, Nellie I Hansen, Rosemary D Higgins, Eunice Kennedy Shriver. Neonatal outcomes of extremely preterm infants from the NICHD Neonatal Research Network. Pediatrics. 2010 Sep; 126(3): 443-56. PMID: 20732945 PMCID: PMC2982806
https://doi.org/10.1542/peds.2009-2959
|
| [17] |
Alana J Westover, Timothy J M Moss. Effects of intrauterine infection or inflammation on fetal lung development. Clin Exp Pharmacol Physiol. 2012 Sep; 39(9): 824-30 PMID: 22816773
https://doi.org/10.1111/j.1440-1681.2012.05742.x
|
| [18] |
Committee on Fetus and Newborn; American Academy of Pediatrics. Respiratory support in preterm infants at birth. Pediatrics. 2014; 133(1): 171-174.
|
| [19] |
Walter-Nicolet E, Courtois E, Milesi C, et al. Premedication practices for delivery room intubations in premature infants in France: Results from the EPIPAGE 2 cohort study. PLoS One. 2019; 14(4): e0215150.
https://doi.org/10.1371/journal.pone.0215150
|
| [20] |
Pladys P, Berneau P, Beuchée A. Modalités non invasives d’instillation du surfactant exogène. /data/revues/0929693X/v22i5sS1/S0929693X15300518/ [Internet]. 2015 Jun 23; PMID: 26112542
https://doi.org/10.1016/S0929-693X(15)30051-8
|
| [21] |
Sweet DG, Carnielli V, Greisen G, et al. European Consensus Guidelines on the Management of Respiratory Distress Syndrome - 2019 Update. Neonatology. 2019; 115(4): 432-450. PMID: 36863329 PMCID: PMC10064400
https://doi.org/10.1159/000528914
|
| [22] |
Stevens TP, Harrington EW, Blennow M et al. Early surfactant administration with brief ventilation vs. selective surfactant and continued mechanical ventilation for preterm infants with or at risk for respiratory distress syndrome. Cochrane Database Syst Rev. 2007; (4): CD003063. PMID: 17943779 PMCID: PMC8554819
https://doi.org/10.1002/14651858.CD003063.pub3
|
| [23] |
Kanmaz HG, Erdeve O, Canpolat FE et al. Surfactant administration via thin catheter during spontaneous breathing: randomized controlled trial. Pediatrics. 2013; 131(2): e502-e509. PMID: 23359581
https://doi.org/10.1542/peds.2012-0603
|
| [24] |
Aldana-Aguirre JC, Pinto M, Featherstone RM et al. Less invasive surfactant administration versus intubation for surfactant delivery in preterm infants with respiratory distress syndrome: a systematic review and meta-analysis. Arch Dis Child Fetal Neonatal Ed. 2017; 102(1): F17-F23. PMID: 27852668
https://doi.org/10.1136/archdischild-2015-310299
|
| [25] |
S J Stock, A J Thomson, S Papworth Antenatal Corticosteroids to Reduce Neonatal Morbidity and Mortality Green–top Guideline No. 7 October 2010. Royal College of Obstetricians and Gynaecologists. PMID: 35172391
https://doi.org/10.1111/1471-0528.17027
|
| [26] |
M Kinalski, A Sledziewski, A Kretowski. Intrauterine stimulation for fetal respiratory system maturation; benefits and risks. Wiad Lek. 2000; 53(9-10): 538-45 PMID: 11148922.
|
| [27] |
D Roberts, S Dalziel. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst Rev 2006; (3): CD004454. PMID: 16856047
https://doi.org/10.1002/14651858.CD004454.pub2
|
| [28] |
Natalia Saldaña-García, María Gracia Espinosa-Fernández, Celia Gómez-Robles et al. Benefits of a Single Dose of Betamethasone in Imminent Preterm Labour. J Clin Med. 2022 Jan; 11(1): 20. PMID: 35011761 PMCID: PMC8745219
https://doi.org/10.3390/jcm11010020
|
| [29] |
David M Haas, William McCullough, Michael F McNamara, Cara Olsen. The first 48 hours: Comparing 12-hour and 24-hour betamethasone dosing when preterm deliveries occur rapidly. J Matern Fetal Neonatal Med. 2006 Jun; 19(6): 365-9. PMID: 16801314
https://doi.org/10.1080/14767050600715873
|
| [30] |
Joonho Lee, Hyo Suk Seong. Evidence to support that spontaneous preterm labor is adaptive in nature: neonatal RDS is more common in "indicated" than in "spontaneous" preterm birth. J Perinat Med. 2009; 37(1): 53-8. PMID: 19099368 PMCID: PMC2887663
https://doi.org/10.1515/JPM.2009.036
|
| [31] |
Fernanda Machado Regazzi, Beatriz Melo Justo. Prenatal or postnatal corticosteroids favor clinical, respiratory, metabolic outcomes and oxidative balance of preterm lambs corticotherapy for premature neonatal lambs. Theriogenology, Volume 182, 1 April 2022, Pages 129-137. PMID: 35168015
https://doi.org/10.1016/j.theriogenology.2022.02.006
|
| [32] |
Tridente A, De Martino L, De Luca D. Porcine vs bovine surfactant therapy for preterm neonates with RDS: systematic review with biological plausibility and pragmatic meta-analysis of respiratory outcomes. Respir Res. 2019; 20(1): 28. PMID: 30728009 PMCID: PMC6366095
https://doi.org/10.1186/s12931-019-0979-0
|
| [33] |
Lamboley-Gilmert G, Lacaze-Masmonteil T; Neonatologists of the Curosurf Postmarketing French Study. The short-term outcome of a large cohort of very preterm infants treated with poractant alfa (Curosurf) for respiratory distress syndrome. A postmarketing phase IV study. Paediatr Drugs. 2003; 5(9): 639-645. PMID: 12956620
https://doi.org/10.2165/00148581-200305090-00006
|
| [34] |
O Baud, L Foix-L'Helias, M Kaminski et al. Antenatal glucocorticoid treatment and cystic periventricular leukomalacia in very premature infants. N Engl J Med. 1999 Oct 14; 341(16): 1190-6. PMID: 10519896
https://doi.org/10.1056/NEJM199910143411604
|
| [35] |
W I Anyaegbunam, A B Adetona. Use of antenatal corticosteroids for fetal maturation in preterm infants. Am Fam Physician. 1997 Sep 15; 56(4): 1093-6 PMID: 9310061.
|
Cite This Article
-
APA Style
Mansour, S., Harb, R., Michel, P., Raymond, S. C., Borrhomée, S. (2024). Complete Versus Incomplete Antenatal Corticosteroid Therapy and Number of Doses of Surfactant Used Posnatally: A Single-Center Study. American Journal of Pediatrics, 10(2), 81-95. https://doi.org/10.11648/j.ajp.20241002.16
 Copy
|
Copy
|
 Download
Download
ACS Style
Mansour, S.; Harb, R.; Michel, P.; Raymond, S. C.; Borrhomée, S. Complete Versus Incomplete Antenatal Corticosteroid Therapy and Number of Doses of Surfactant Used Posnatally: A Single-Center Study. Am. J. Pediatr. 2024, 10(2), 81-95. doi: 10.11648/j.ajp.20241002.16
Copy
|
Download
AMA Style
Mansour S, Harb R, Michel P, Raymond SC, Borrhomée S. Complete Versus Incomplete Antenatal Corticosteroid Therapy and Number of Doses of Surfactant Used Posnatally: A Single-Center Study. Am J Pediatr. 2024;10(2):81-95. doi: 10.11648/j.ajp.20241002.16
Copy
|
Download
-
@article{10.11648/j.ajp.20241002.16,
author = {Suzi Mansour and Rami Harb and Philippe Michel and Sarah Cassandra Raymond and Suzanne Borrhomée},
title = {Complete Versus Incomplete Antenatal Corticosteroid Therapy and Number of Doses of Surfactant Used Posnatally: A Single-Center Study
},
journal = {American Journal of Pediatrics},
volume = {10},
number = {2},
pages = {81-95},
doi = {10.11648/j.ajp.20241002.16},
url = {https://doi.org/10.11648/j.ajp.20241002.16},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajp.20241002.16},
abstract = {Introduction: Antenatal corticosteroid therapy reduces the risk of developing RDS in premature infants. A single complete course of two doses of betamethasone is recommended between 24 weeks and 34 weeks. There are few data on the neonatal effects of an incomplete course of antenatal corticosteroid therapy. The main objective of our study is to evaluate the effectiveness of a complete versus incomplete course of antenatal corticosteroid therapy on the number of doses of surfactant received postnatally. Methods: This is a single-center retrospective study, including 145 newborns with RDS, divided into 2 groups according to the number of doses of antenatal corticosteroid therapy (1 dose; n = 23 and 2 doses; n = 95). Results: The clinical characteristics of the newborns were similar in the 2 groups. The number of doses of surfactants received postnatally and the severity of RDS are not influenced by the number of doses of antenatal corticosteroid therapy. On the other hand, the number of doses of surfactants received is influenced by the term of birth, the presence of an neonatal sepsis and by resuscitation in the delivery room. The severity of RDS is not influenced either by the interval between the last dose of antenatal corticosteroid therapy and delivery, nor by the cause of prematurity. We did not note any statistically significant difference in clinical improvement (duration of intubation, duration of non-invasive ventilation), the need for postnatal corticosteroid therapy and the risk of occurrence of morbidity and mortality (mortality rate, occurrence of BPD, IVH, severe NEC) between the two groups. Conclusion: just like a complete course, an incomplete course of antenatal corticosteroid therapy can also act on the severity of RDS. Prospective randomized studies should be considered for a formal determination of the neonatal effects of a complete versus incomplete course of antenatal corticosteroid therapy, including the trial BETADOSE.
},
year = {2024}
}
Copy
|
Download
-
TY - JOUR
T1 - Complete Versus Incomplete Antenatal Corticosteroid Therapy and Number of Doses of Surfactant Used Posnatally: A Single-Center Study
AU - Suzi Mansour
AU - Rami Harb
AU - Philippe Michel
AU - Sarah Cassandra Raymond
AU - Suzanne Borrhomée
Y1 - 2024/04/28
PY - 2024
N1 - https://doi.org/10.11648/j.ajp.20241002.16
DO - 10.11648/j.ajp.20241002.16
T2 - American Journal of Pediatrics
JF - American Journal of Pediatrics
JO - American Journal of Pediatrics
SP - 81
EP - 95
PB - Science Publishing Group
SN - 2472-0909
UR - https://doi.org/10.11648/j.ajp.20241002.16
AB - Introduction: Antenatal corticosteroid therapy reduces the risk of developing RDS in premature infants. A single complete course of two doses of betamethasone is recommended between 24 weeks and 34 weeks. There are few data on the neonatal effects of an incomplete course of antenatal corticosteroid therapy. The main objective of our study is to evaluate the effectiveness of a complete versus incomplete course of antenatal corticosteroid therapy on the number of doses of surfactant received postnatally. Methods: This is a single-center retrospective study, including 145 newborns with RDS, divided into 2 groups according to the number of doses of antenatal corticosteroid therapy (1 dose; n = 23 and 2 doses; n = 95). Results: The clinical characteristics of the newborns were similar in the 2 groups. The number of doses of surfactants received postnatally and the severity of RDS are not influenced by the number of doses of antenatal corticosteroid therapy. On the other hand, the number of doses of surfactants received is influenced by the term of birth, the presence of an neonatal sepsis and by resuscitation in the delivery room. The severity of RDS is not influenced either by the interval between the last dose of antenatal corticosteroid therapy and delivery, nor by the cause of prematurity. We did not note any statistically significant difference in clinical improvement (duration of intubation, duration of non-invasive ventilation), the need for postnatal corticosteroid therapy and the risk of occurrence of morbidity and mortality (mortality rate, occurrence of BPD, IVH, severe NEC) between the two groups. Conclusion: just like a complete course, an incomplete course of antenatal corticosteroid therapy can also act on the severity of RDS. Prospective randomized studies should be considered for a formal determination of the neonatal effects of a complete versus incomplete course of antenatal corticosteroid therapy, including the trial BETADOSE.
VL - 10
IS - 2
ER -
Copy
|
Download