Objective: To explore the clinicopathological characteristics of spiradenoma (SA), and make exact diagnosis and differential diagnosis of this disease. Methods: The clinical and pathological data of 11 patients with spiradenoma in the First Affiliated Hospital of Jinan University from 2013 to 2022 were retrospectively analyzed, and combined with the review of literatures. Results: Among the 11 patients with spiroadenomas, 6 cases were male and 5 were female; the age ranged from 19 to 70 years old, with an average age of 41 years; Spiradenomas are more common in the trunk and limbs. At low-power microscope, the tumor mass with capsule in the dermis. Under a high-power microscope, the tumor is usually composed of two types of cells, which are the marginal small basaloid cells with dark staining and central larger cells with a pale and acidophilic nucleus. Other morphological structures included 2 cases of cystic solid and cylindroma respectively. Immunohistochemistry showed that epithelial and myoepithelial differentiation. Conclusion: Spiradenoma often occurs subcutaneously and requires histopathological diagnosis to avoid misdiagnosis. Its biological behavior is benign and its prognosis is good. But malignant transformation should be considered in some case with long course or relapses. SA is rare in clinical and is prone to misdiagnosis or missed diagnosis. This study summarizes the clinilcopathological characteristics of SA, providing reference for future clinical diagnosis and treatment.
| Published in | American Journal of Clinical and Experimental Medicine (Volume 12, Issue 2) |
| DOI | 10.11648/j.ajcem.20241202.11 |
| Page(s) | 8-12 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Spiradenoma, Pathological Features, Differential Diagnosis
2.1. Materials
2.2. Methods
3.1. Clinical Characteristics
3.2. Clinical Features
3.3. Pathological Features
3.4. Immunohistochemical
3.5. Treatment and Prognosis
| [1] | Kersting D W, Helwig E B. Eccrine spiradenoma [J]. AMA Arch Derm, 1956, 73(3): 199-227. |
| [2] | Dhua S, Sekhar D R. A rare case of eccrine spiradenoma-treatment and management [J]. Eur J Plast Surg, 2016, 39: 143-146. |
| [3] | Clarke J, Ioffreda M, Helm KF. Multiple familial trichoepitheliomas: a folliculosebaceous-apocrine genodermatosis. Am J Dermatopathol. 2002 Oct; 24(5): 402-5. |
| [4] | Dabska M. Malignant transformation of eccrine spiradenoma [J]. Pol Med J, 1972, 11(2): 388-396. |
| [5] | Chow W, Griffiths M. A malignant eccrine spiradenoma of the scalp. BMJ Case Rep. 2014 May 19; 2014: bcr2013202524. |
| [6] | Tiradogonzalez M, Beierle E, Hammers Y, Andea A, and Mroczek E. Neonatal spiradenoma [J]. Pediatr Dermatol, 2013, 30(6): e228-229. |
| [7] | Guzelbey B, Leblebici C, Baykal Koca S. Eccrine spiradenoma mimicking adenoid cystic carcinoma cytologically (two case reports and literature review) [J]. Diagn Cytopathol, 2022, 50(1): E6-e12. |
| [8] | Metovic J, Gallino C, Zanon E, Bussone R, Russo R, Vissio E, et al. Eccrine spiradenoma of the nipple: Case report, differential diagnosis and literature review [J]. Histol Histopathol, 2019, 34(8): 909-915. |
| [9] | Cukic O, Jovanovic M B, Milutinovic Z. An unusual nodule on the auricle: Eccrine spiradenoma [J]. Ear Nose Throat J, 2019, 98(9): 545-546. |
| [10] | Hao Zhang, Xian Hu, Xiaoling Wang, Lele Sun, Yongxia Liu, Hong Liu. Detection of cyld gene mutation in a family with multiple familial trichoepithelioma and literature review [J]. Chin J Derm Venereol, 2019: 33(11): 1247-1250. |
| [11] | Kanwaljeet S, Chatterjee T. Eccrine spiradenoma: A rare adnexal tumor [J]. Indian J Cancer, 2017, 54(4): 695-696. |
| [12] | Salim S, Bounniyt H, El Amraoui M, Benzekri A, Senouci K, and Hassam B. Malignant transformation of a spiradenoma with blaschkoïd pattern [J]. Clin Case Rep, 2018, 6(11): 2086-2088. |
| [13] | Staiger R D, Helmchen B, Papet C, Mattiello D, and Zingg U. Spiradenocarcinoma: A comprehensive data review [J]. Am J Dermatopathol, 2017, 39(10): 715-725. |
| [14] | Feini Xu, Aijun Chen. Analysis of clinical and pathological features of 14 patients with eccrine spiradenoma [J] Chian Journal of Leprosy and Skin Diseases, 2021, 37(07): 424-427. |
| [15] | Jacquemus J, Dalle S, Faure M, Chouvet B, Beatrix O, and Balme B. [malignant transformation of an eccrine spiradenoma] [J]. Ann Dermatol Venereol, 2017, 144(3): 203-207. |
| [16] | Huang A, Vyas N S, Mercer S E, and Phelps R G. Histological findings and pathologic diagnosis of spiradenocarcinoma: A case series and review of the literature [J]. J Cutan Pathol, 2019, 46(4): 243-250. |
| [17] | Wagner K, Jassal K, Lee J C, Ban E J, Cameron R, and Serpell J. Challenges in diagnosis and management of a spiradenocarcinoma: A comprehensive literature review [J]. ANZ J Surg, 2021, 91(10): 1996-2001. |
| [18] | Wargo J J, Carr D R, Plaza J A, and Verschraegen C F. Metastatic spiradenocarcinoma managed with pd-1 inhibition [J]. J Natl Compr Canc Netw, 2022: 1-3. |
APA Style
Tian, Q., Hu, Y., Lu, Y. (2024). Clinicopathological Characteristics of 11 Cases with Spiradenoma: A Rare Adnexal Tumor. American Journal of Clinical and Experimental Medicine, 12(2), 8-12. https://doi.org/10.11648/j.ajcem.20241202.11
ACS Style
Tian, Q.; Hu, Y.; Lu, Y. Clinicopathological Characteristics of 11 Cases with Spiradenoma: A Rare Adnexal Tumor. Am. J. Clin. Exp. Med. 2024, 12(2), 8-12. doi: 10.11648/j.ajcem.20241202.11
AMA Style
Tian Q, Hu Y, Lu Y. Clinicopathological Characteristics of 11 Cases with Spiradenoma: A Rare Adnexal Tumor. Am J Clin Exp Med. 2024;12(2):8-12. doi: 10.11648/j.ajcem.20241202.11
@article{10.11648/j.ajcem.20241202.11,
author = {Qianyuan Tian and Yunfeng Hu and Yuanzhi Lu},
title = {Clinicopathological Characteristics of 11 Cases with Spiradenoma: A Rare Adnexal Tumor
},
journal = {American Journal of Clinical and Experimental Medicine},
volume = {12},
number = {2},
pages = {8-12},
doi = {10.11648/j.ajcem.20241202.11},
url = {https://doi.org/10.11648/j.ajcem.20241202.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajcem.20241202.11},
abstract = {Objective: To explore the clinicopathological characteristics of spiradenoma (SA), and make exact diagnosis and differential diagnosis of this disease. Methods: The clinical and pathological data of 11 patients with spiradenoma in the First Affiliated Hospital of Jinan University from 2013 to 2022 were retrospectively analyzed, and combined with the review of literatures. Results: Among the 11 patients with spiroadenomas, 6 cases were male and 5 were female; the age ranged from 19 to 70 years old, with an average age of 41 years; Spiradenomas are more common in the trunk and limbs. At low-power microscope, the tumor mass with capsule in the dermis. Under a high-power microscope, the tumor is usually composed of two types of cells, which are the marginal small basaloid cells with dark staining and central larger cells with a pale and acidophilic nucleus. Other morphological structures included 2 cases of cystic solid and cylindroma respectively. Immunohistochemistry showed that epithelial and myoepithelial differentiation. Conclusion: Spiradenoma often occurs subcutaneously and requires histopathological diagnosis to avoid misdiagnosis. Its biological behavior is benign and its prognosis is good. But malignant transformation should be considered in some case with long course or relapses. SA is rare in clinical and is prone to misdiagnosis or missed diagnosis. This study summarizes the clinilcopathological characteristics of SA, providing reference for future clinical diagnosis and treatment.
},
year = {2024}
}
TY - JOUR T1 - Clinicopathological Characteristics of 11 Cases with Spiradenoma: A Rare Adnexal Tumor AU - Qianyuan Tian AU - Yunfeng Hu AU - Yuanzhi Lu Y1 - 2024/04/11 PY - 2024 N1 - https://doi.org/10.11648/j.ajcem.20241202.11 DO - 10.11648/j.ajcem.20241202.11 T2 - American Journal of Clinical and Experimental Medicine JF - American Journal of Clinical and Experimental Medicine JO - American Journal of Clinical and Experimental Medicine SP - 8 EP - 12 PB - Science Publishing Group SN - 2330-8133 UR - https://doi.org/10.11648/j.ajcem.20241202.11 AB - Objective: To explore the clinicopathological characteristics of spiradenoma (SA), and make exact diagnosis and differential diagnosis of this disease. Methods: The clinical and pathological data of 11 patients with spiradenoma in the First Affiliated Hospital of Jinan University from 2013 to 2022 were retrospectively analyzed, and combined with the review of literatures. Results: Among the 11 patients with spiroadenomas, 6 cases were male and 5 were female; the age ranged from 19 to 70 years old, with an average age of 41 years; Spiradenomas are more common in the trunk and limbs. At low-power microscope, the tumor mass with capsule in the dermis. Under a high-power microscope, the tumor is usually composed of two types of cells, which are the marginal small basaloid cells with dark staining and central larger cells with a pale and acidophilic nucleus. Other morphological structures included 2 cases of cystic solid and cylindroma respectively. Immunohistochemistry showed that epithelial and myoepithelial differentiation. Conclusion: Spiradenoma often occurs subcutaneously and requires histopathological diagnosis to avoid misdiagnosis. Its biological behavior is benign and its prognosis is good. But malignant transformation should be considered in some case with long course or relapses. SA is rare in clinical and is prone to misdiagnosis or missed diagnosis. This study summarizes the clinilcopathological characteristics of SA, providing reference for future clinical diagnosis and treatment. VL - 12 IS - 2 ER -
Department of Dermatology, First Affiliated Hospital of Ji’nan University, Guangzhou, China
Department of Dermatology, First Affiliated Hospital of Ji’nan University, Guangzhou, China
Department of Pathology, First Affiliated Hospital of Ji’nan University, Guangzhou, China
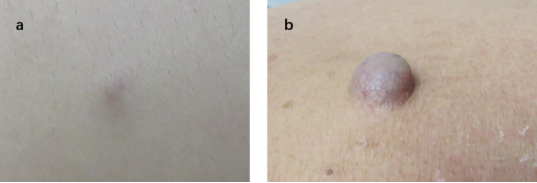
Figure 1. (a-b): Clinical manifestations of SA: normal skin color and bule papules.
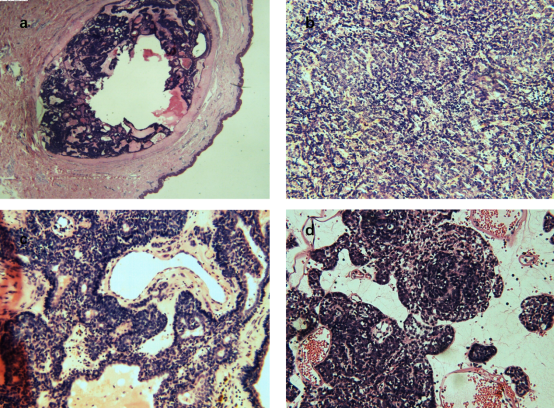
Figure 2. (a-d): Hematoxylin & Eosin-stained: a: the tumor is located within the dermis and surrounded by the capsule (HE × 40); b: tumor cells showing rosette-like arrangement of the two-cell population: small dark and basaloid cells with hyperchromatic nuclei and larger cells with a pale nucleus (HE × 100); c: prominent deposition of eosinophilic basement membrane- like material and focal duct formation were noted (HE × 200); d: vascular lumen filled with red blood cells (HE × 200).
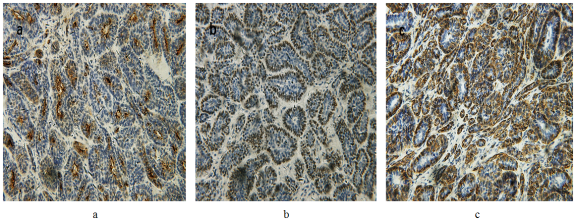
Figure 3. (a-c): Immunohistochemical -stained: positive staining: a: EMA: expression of sweat gland lumen marker highlighted the central cells (IHC × 200); b-c: SMA, p63: expression of myoepithelial marker highlighted the small-sized cells with dark chromatin (IHC × 200).
Information

